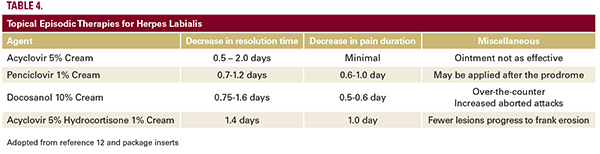
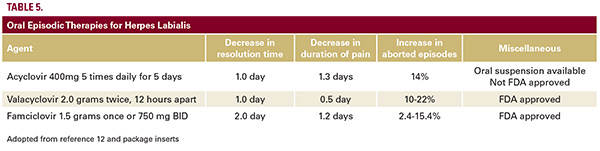
 the clinical benefits from episodic topical therapy are modest. While topical drugs are quite safe, such agents are also very inconvenient, as they are require frequent and prolonged application. Acyclovir cream approved use is five times daily for four days; penciclovir cream is to be applied every two hours while awake for four days; docosanol cream is five times daily “until healed”; and acyclovir-hydrocortisone cream indicated dosage is 5 times daily for 5 days. The newest of the approved topical agents, acyclovir 5%-hydrocortisone 1% cream, was first introduced in 2009, and theoretically uniquely addresses both symptomatic relief and healing by concurrently reducing inflammation while exerting direct anti-viral effects.17 Two unique benefits related to this agent compared to placebo are smaller ultimate mean lesional size and fewer outbreaks progressing to overt erosion.17 An interesting adaptation of the aforementioned steroid/anti-viral combination as episodic therapy was tested on 42 patients, wherein a placebo-placebo group was compared to subjects who received valacyclovir (2 g orally BID for 1 day) and topical clobetasol gel 0.05% (BID for 3 days applied to the affected area).18 Patients who received the combination therapy experienced more aborted lesions (50% versus 15.8%), a reduced the mean maximum lesion size (9.7 versus 54 mm) and most strikingly a lower mean healing time of classical lesions (5.8 versus 9.3 days).18 This regimen, while proving quite effective in a small randomized and controlled study, did not alter the long-term natural disease history. A different, similarly sized (n=49) study compared oral famciclovir 500 mg and topical fluocinonide .05% gel, administered three times daily for five days, to oral famciclovir and gel vehicle dosed in the same manner. In this steroid/anti-viral comparison to an active anti-viral agent plus placebo, addition of the steroid proved beneficial on some efficacy parameters; namely, the topical steroid/oral anti-viral subjects experienced: more aborted lesions, reduced maximum lesion size, and non-statistically significant reduced duration of pain and reduced healing time.19 Based on just a few studies, it appears that the addition of a topical corticosteroid to antiviral therapy produces improvements in the clinical course of herpes labialis, compared to antiviral agent monotherapy, and that such combination therapy shows an even greater degree of benefit compared to no treatment.What about episodic oral anti-viral therapy? The most typically utilized oral therapies are summarized in Table 5. For all these regimens to be successful, drug is best taken within one hour of the onset of a prodrome. In patients lacking a definable prodrome, drug should be taken within 48 hours of the onset of any sign or symptom (eg, erythema, papule, or vesicle formation). As is true of topical therapy, episodic treatment with oral anti-viral drugs provides modest improvements in time to lesion healing and duration of pain. It should be noted that acyclovir is relatively insoluble in urine, is rapidly filtered by glomeruli and secreted by renal tubules, thereby producing high urinary concentrations, especially in patients with pre-existing renal impairment.20 In turn, this may lead to direct renal tubular toxicity, acute interstitial nephritis and/or crystal nephropathy.21 While the absolute risk is certainly small (less than 0.5%) and discontinuation
the clinical benefits from episodic topical therapy are modest. While topical drugs are quite safe, such agents are also very inconvenient, as they are require frequent and prolonged application. Acyclovir cream approved use is five times daily for four days; penciclovir cream is to be applied every two hours while awake for four days; docosanol cream is five times daily “until healed”; and acyclovir-hydrocortisone cream indicated dosage is 5 times daily for 5 days. The newest of the approved topical agents, acyclovir 5%-hydrocortisone 1% cream, was first introduced in 2009, and theoretically uniquely addresses both symptomatic relief and healing by concurrently reducing inflammation while exerting direct anti-viral effects.17 Two unique benefits related to this agent compared to placebo are smaller ultimate mean lesional size and fewer outbreaks progressing to overt erosion.17 An interesting adaptation of the aforementioned steroid/anti-viral combination as episodic therapy was tested on 42 patients, wherein a placebo-placebo group was compared to subjects who received valacyclovir (2 g orally BID for 1 day) and topical clobetasol gel 0.05% (BID for 3 days applied to the affected area).18 Patients who received the combination therapy experienced more aborted lesions (50% versus 15.8%), a reduced the mean maximum lesion size (9.7 versus 54 mm) and most strikingly a lower mean healing time of classical lesions (5.8 versus 9.3 days).18 This regimen, while proving quite effective in a small randomized and controlled study, did not alter the long-term natural disease history. A different, similarly sized (n=49) study compared oral famciclovir 500 mg and topical fluocinonide .05% gel, administered three times daily for five days, to oral famciclovir and gel vehicle dosed in the same manner. In this steroid/anti-viral comparison to an active anti-viral agent plus placebo, addition of the steroid proved beneficial on some efficacy parameters; namely, the topical steroid/oral anti-viral subjects experienced: more aborted lesions, reduced maximum lesion size, and non-statistically significant reduced duration of pain and reduced healing time.19 Based on just a few studies, it appears that the addition of a topical corticosteroid to antiviral therapy produces improvements in the clinical course of herpes labialis, compared to antiviral agent monotherapy, and that such combination therapy shows an even greater degree of benefit compared to no treatment.What about episodic oral anti-viral therapy? The most typically utilized oral therapies are summarized in Table 5. For all these regimens to be successful, drug is best taken within one hour of the onset of a prodrome. In patients lacking a definable prodrome, drug should be taken within 48 hours of the onset of any sign or symptom (eg, erythema, papule, or vesicle formation). As is true of topical therapy, episodic treatment with oral anti-viral drugs provides modest improvements in time to lesion healing and duration of pain. It should be noted that acyclovir is relatively insoluble in urine, is rapidly filtered by glomeruli and secreted by renal tubules, thereby producing high urinary concentrations, especially in patients with pre-existing renal impairment.20 In turn, this may lead to direct renal tubular toxicity, acute interstitial nephritis and/or crystal nephropathy.21 While the absolute risk is certainly small (less than 0.5%) and discontinuation
