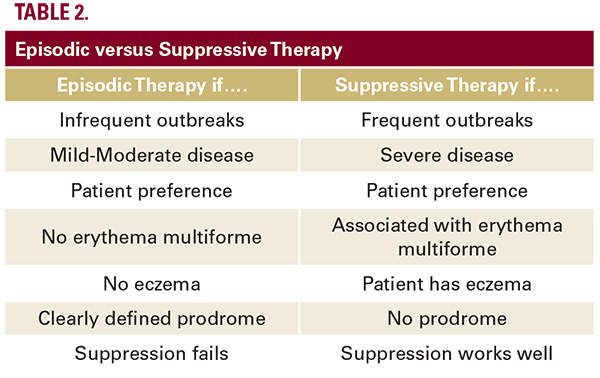
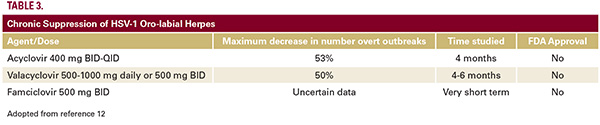
Primary Herpetic Gingivo-StomatitisAlthough discussion of this entity, most often seen in the pediatric population, is beyond the scope and purpose of this paper, the typical treatment options are shown in Table 1. Please note that the safety and efficacy of the commonly used oral anti-herpes drugs (acyclovir and its analogues) have not been established in the population under 12 years of age; therefore, formal FDA approval does not exist.12Recurrent Oro-Labial Herpes: Suppressive TherapyIn managing recurrent HSV-1, there are several key decisions. Most importantly, the clinician must decide between episodic treatment (only administered during an outbreak) or chronic suppressive treatment. Episodic therapy can be accomplished via topical, systemic, and mucosal routes of drug administration, whereas chronic suppressive therapy is primarily accomplished by oral anti-viral drug administration. Some possible reasons to choose episodic or suppressive therapy are enumerated in Table 2, with the caveats that therapeutic choices Rosenmust always be individualized and selected by the healthcare provider following thorough discussion with the patient. Anti-viral drug dosages frequently utilized in chronic suppression are shown in Table 3. However, none of these regimens are FDA approved, and chronic anti-viral drug suppression of HSV-1 with resultant reduction in clinical outbreaks is much more difficult to successfully achieve than with HSV-2-related genital herpes.12,13 As aptly summarized in a recent Cochrane Systematic Review: “The current evidence demonstrates that long-term use of oral antiviral agents can prevent HSL (herpes simplex labialis), but the clinical benefit is small.”14 Acyclovir has also been associated with several different forms of nephrotoxicity; this problem is discussed below. A host of other potential interventions designed to prevent herpes labialis outbreaks (such as oral lysine, ingestion of various food supplements, low-level laser therapy, administration of gamma globulin, or yellow fever vaccine) have not proven successful.14 The use of topical imiqumod, when applied directly to the lesion as an attempt to meaningfully suppress herpes labialis, has largely been abandoned due to the potential for a severe local reaction.15 However, an intriguing case report detailed the once daily occlusive application of ¼ a standard sachet of 5% imiquimod to a distant skin site for three weeks, with the treatment starting during an active outbreak.16 This method resulted in a massive polarized Th-1 immune response with interferon-γ release, and notable clinical suppression: namely, a remission of one and a half years duration.16 Unfortunately, there have been no confirmatory or follow-up reports regarding this method of attaining disease suppression. Recurrent Oro-Labial Herpes: Episodic Therapy As noted previously, there exists a plethora of therapeutic choices for the episodic management of oro-labial herpes. It should be noted that all episodic interventions demonstrate optimal benefit when administered immediately upon onset of the outbreak prodrome. Topical therapies are listed in Table 4. Why might topical therapy be preferred by select patients? Some reasons include: few real or potential side effects in the short-term and no long-term health concerns; no drug-drug interactions to consider; easy portability and rapid initiation; application right to the site of cutaneous pathology giving the patient a feeling of empowerment; and cost-effectiveness. However, even a cursory glance at Table 4 shows that