The pathogenesis of eczema is both complex and multifactorial.3 However, eczema-prone skin is susceptible to dysbiosis and weakened epidermal barrier function, and exposure to small irritant or allergens can stimulate disease flares.3,6-8 Because eczema affects the skin barrier, which has a primary function of restricting water loss and preventing the entry of irritants/allergens, supporting skin barrier function is essential.3
Utilization of a skincare regimen targeted to eczema-prone skin can be a cost-effective way to minimize symptom flares along with trigger avoidance. This study evaluated a 3-step over-the-counter (OTC) regimen consisting of an itch relief gel, flare relief cream, and a soothing moisturizer. The goal of this regimen is to relieve itch and thereby break the itch/scratch cycle of eczema. It was also designed to support and repair skin barrier function while relieving eczema symptoms, as well as to minimize the occurrence of flares in order to improve QoL.
MATERIALS AND METHODS
This was a multicenter, 12-week in-use study of a skincare regimen in patients with eczema and was conducted between March 2, 2022 and February 2, 2023. The test regimen included 3 products: itch relief gel for itchy areas, cream all over face/body, and a moisturizer for eczema-affected areas (Cetaphil® Restoraderm, Galderma Laboratories LP, Dallas, TX). Participants were also allowed to use a neutral cleanser and moisturizer as well as a soothing wash. The study was reviewed and approved by Advarra Institutional Review Board (IRB), followed Good Clinical Practice, and all subjects provided written informed consent.
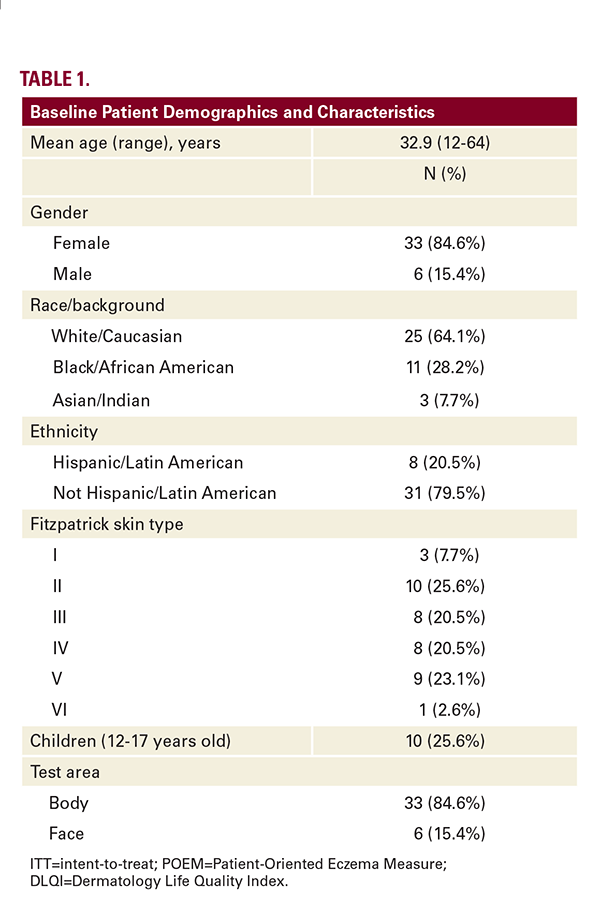
Patients were eligible to participate if they were aged 12 years and older, inclusive of any Fitzpatrick skin phototypes and any race/ethnicity, and had a score of 6 to 16 on the Patient Oriented Eczema Measure (POEM) questionnaire (mild-to-moderate severity) at screening and baseline. To be eligible, patients also had to have experienced at least 2 flares (defined as a return of eczema symptoms including worsening skin rash) within the 3 months prior to screening with the latest flare occurring within 6 weeks of baseline visit. Participants used a neutral cleanser and moisturizer for 5 to 14 days upon the screening period, then switched to the test regimen at baseline for the remaining study. Participants were also allowed to use 1% hydrocortisone if their eczema flare-up was uncontrolled and/or unbearably itchy.
Efficacy assessments included the Eczema Area and Severity Index (EASI, scores range from 0=no disease anywhere on the body to 72=most severe disease on all body areas) and the Patient-Oriented Eczema Measure (POEM, 0=clear to 28=very severe), both performed at baseline and weeks 4, 8, and 12. Digital photography was also performed. Participants also completed self-assessment questionnaires, including the validated ItchyQuant Assessment (numerical rating scale from 0=none to 10=worst itch imaginable), the Dermatology Life Quality Index (DLQI, 0=no effect at all to 30=extremely large effect), and a satisfaction questionnaire.
Safety was assessed by tolerability evaluations of burning and stinging (0=none to 3=severe) at baseline and weeks 4, 8, and 12 as well as collection of adverse events for participants who qualified with active lesions and/or dry patches on the face or body.
Statistics included demographic and baseline characteristics, descriptive statistics for continuous variables, and the frequency and percentage per category for categorical variables. Number of flares was summarized for each time point and the total number occurring from baseline to week 12 was compared with the number of flares experienced during the 3 months prior to screening. The Wilcoxon signed-rank test was used to analyze change from baseline and all statistical tests were 2-sided at significance level alpha=0.05. Questionnaire data were tabulated, and the frequency and percentage of all responses were reported.
RESULTS
Forty patients qualified for the study and one discontinued (for a total of 39 participants in the intent to treat [ITT] population); 34 completed all study visits per protocol. Patient demographics and

