 study was to determine which factors significantly impact clinicians’ decisions to utilize the 31-GEP test to predict metastatic risk in patients with cutaneous malignant melanoma.
study was to determine which factors significantly impact clinicians’ decisions to utilize the 31-GEP test to predict metastatic risk in patients with cutaneous malignant melanoma. METHODS
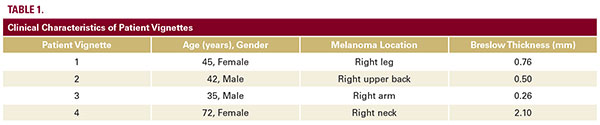
Attendees at a national dermatology conference were sequentially presented with four patient vignettes, each a case of cutaneous malignant melanoma with a different Breslow thickness (Table 1). For each vignette, respondents were asked, via an anonymous audience response system, whether they would recommend the 31-GEP test for the patient. They were then asked to consider whether they would recommend the test for the same patient under two specific situations: 1) if the lesion were ulcerated and 2) if the patient had a negative sentinel lymph node biopsy. Respondents were also asked whether 31-GEP test results would affect their decision to recommend sentinel lymph node biopsy (SLNBx) in patients with 0.76-1.0 mm thick tumorsAdditional questions were asked about years of clinical experience and previous familiarity with the 31-GEP test. Summary statistics were calculated for demographic variables. Chi-squared tests were used for comparison, with a P-value of P<0.05 considered significant. All analyses were performed using STATA statistical software (Version 15, College Station, TX). This study was Institutional Review Board exempt.
RESULTS
Sample Characteristics
A total of 181 of 187 individuals completed the survey (96.8% response rate). The sample consisted of mostly practicing dermatologists with relatively few trainees; roughly 50% of the sample had been in practice for more than 20 years. Two-thirds of respondents were previously familiar with the 31-GEP test.
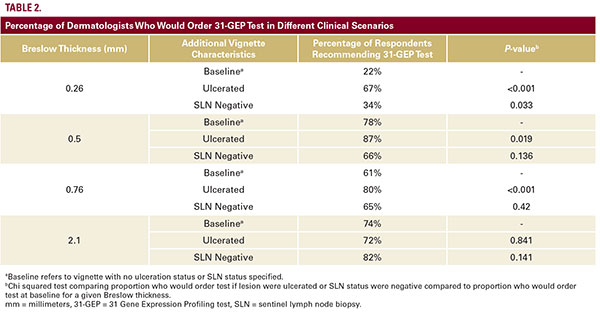
Factors Impacting Clinicians’ Decision to Order 31-GEP Test
For all vignettes with tumors with thickness of 0.5 mm or greater, the majority of respondents would recommend the 31-GEP test (Table 2). Only for the vignette with 0.26 mm tumor did a minority (22%) of subjects say they would recommend the