

of the suture cost.6 For small repairs, often there is Monocryl suture remaining from the first package after deep approximation,
which can be used for superficial closure. However, more often 2 packages of Monocryl are used to close excisions on the trunk; a 3-0 Monocryl for the deep layer and a 5-0 Monocryl for subcuticular running. Nonetheless, on a global scale, the cost of a second package of Monocryl pales in comparison to health care dollars spent on return visits for suture removal.
TECHNIQUE
First, an elliptical excision is performed to the level of subcutaneous
tissue after careful planning and alignment with relaxed skin tension lines (Figure 1). Following undermining and hemo

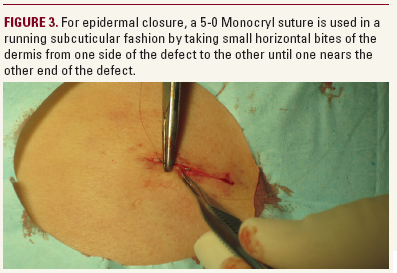
stasis, a 3-0 Monocryl suture is used to approximate the deep layer using subcutaneous interrupted sutures while obtaining eversion and minimizing dead space (Figure 2). This reduces the risk of hematoma and scar stretching. Once the deeper layer is placed, a 5-0 Monocryl running subcuticular suture is used to close the defect. Starting at one end of the ellipse, a subcutaneous suture in placed, a knot is tied, and only the short end of the thread is then cut right above the knot. Next, the long end of the suture is used to run the subcuticular suture, small horizontal bites of the dermis are taken and placed from one side of the defect to the other until one nears the other end of the defect (Figure 3). At that point, the suture is passed from under
the skin in the subcutaneous plane and vertically removed farther away from the incision site, typically about a centimeter. No knots are placed, and the suture thread is cut flush against the skin, leaving a mostly flat, well-approximated linear closure (Figure 4). Steri-Strips (3M, St. Paul, MN) are placed on the wound, followed by a pressure bandage. The advantage of this method is that sutures do not require removal, and more importantly,
the long absorption time for the running subcuticular suture allows the wound to be held together, reducing possibility
of stretching of the apposed tissue.
DISCLOSURES
The authors have no relevant conflicts of interest to disclose.
REFERENCES
- Adams B, Levy R, Rademaker AE, Goldberg LH, Alam M. Frequency of use of suturing and repair techniques preferred by dermatologic surgeons. Dermatol Surg. 2006;32(5):682-689.
- Bennett RG. Selection of wound closure materials. J Am Acad Dermatol. 1988;18(4 Pt 1):619-637.
- Rosenzweig LB, Abdelmalek M, Ho J, Hruza GJ. Equal cosmetic outcomes with 5-0 poliglecaprone-25 versus 6-0 polypropylene for superficial closures. Dermatol Surg. 2010;36(7):1126-1129.
- Monocryl [package insert]. San Angelo, TX: Ethicon, Inc; 1995.
- Moy RL, Waldman B, Hein D. A review of sutures and suturing techniques. J Dermatol Surg Oncol. 1992;18(9):785-795.
- Fosko SW, Heap D. Surgical pearl: an economical means of skin closure with absorbable suture. J Am Acad Dermatol. 1998;39(2 Pt 1):248-250.
AUTHOR CORRESPONDENCE
Jesse M. Lewin MDLewin.jesse@gmail.com

