Atopic dermatitis visits were identified using the ICD-9-CM diagnostic code 691.8 from the years 2006 to 2015. A survey with missing treatment or survey weight and nondermatologic medications were excluded.16 Frequency tables of age, gender, ethnicity, provider treating AD, and treatment regimens were recorded. Although NAMCS mentioned moisturizers in the treatment regimen, moisturizers are not considered a drug and may not have been formally prescribed; therefore, our results may underrepresent physician’s instructions for applying a moisturizer. A more detailed explanation of the methods has been published.16,17 Statistical analysis was calculated by SURVEYFREQ and SURVEYMEANS using SAS 9.4. The frequency of AD visits per 100 white, African American, and Asian American patients were calculated by dividing the estimated total number of AD visits in each racial population by the total racial census population from 2006 to 2015 and multiplied by 100. The census data was obtained from the United States Census Bureau.18 Frequency of AD visits per dermatologist, pediatrician, and family physician was calculated by dividing the total number of AD visits in each specialty by the total population of each specialist from 2006 to 2015. Since we were unable to find the specialist population in 2014, the specialist populations from 2013 and 2015 were added and divided by two to receive an average population in 2014. Since we had access to all specialist populations using the AMA and AAMC database, we deferred calculating the midpoint as we believe we could get a more accurate specialist population from the AMA and AAMC data from 2006 to 2015.19-27 This study was exempt from IRB approval by the Wake Forest Baptist Health Institutional Review Board.
RESULTS
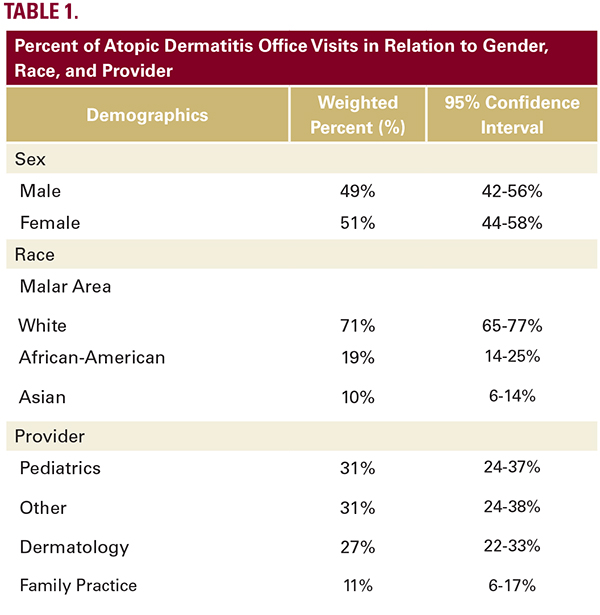
The NAMCS search yielded an estimated 10.4 (95% Confidence Interval [CI]: 9.2, 11.5) million AD office visits from 2006 to 2015. There were approximately an equal number of male visits (51%; 44-58%) and more white race patients (71%; 65-77%) (Table 1). Considering all ambulatory visits from 2006 to 2015, of the white population, 3 out of 1000 ambulatory visits were ADrelated; whereas of the African American and Asian American population, 5 out of 1000 and 7 out of 1000 visits were ADrelated, respectively. The most common provider managing AD were pediatricians (31%; 24-37%) and other providers (31% of total visits; 24-38%), followed by dermatologists (27%; 22-33%), and family physicians (11%; 6-17%) (Table 1). The frequency of AD visits per dermatologist was 25.5 AD visits per pediatrician, and 1 AD visit per family physician.
The most common medication class prescribed was topical corticosteroids (59%; 52-66%), followed by moisturizers (12%; 8-17%), antibiotics (11%; 6-16%), and second generation antihistamines (6%; 3-10%) (Table 2). Triamcinolone was the most common prescribed topical corticosteroid (prescribed at 25% of office visits; 18-31%), followed by hydrocortisone (19%; 14- 24%), desonide (6%; 3-9%), clobetasol (4%; 2-6%), fluocinolone (2%; 1-4%), and desoximetasone (1%; 0-1%) (Table 2). Although moisturizers were mentioned at 12% (8-17%) of AD visits across all age groups, our data may not be a valid observation for moisturizer use. Although moisturizers were mentioned in the NAMCS database, our observations may underrepresent the true physician orders for moisturizer application. Pimecrolimus was prescribed at 6% (1-11%) of visits and cetirizine at 4% (2-7%).