 caused by smoking are associated with poor overall skin quality, which is less likely to achieve the same magnitude of response as healthy skin. To help counter this effect, some advisors provide oral nutritional supplements and vitamins, such as ascorbic acid (vitamin C) to counteract the damaging oxidative effects of smoking and maximize the beneficial effects of MFU-V.Another factor is a high body-mass index (BMI), especially for a single MFU-V treatment. As it is challenging to lift heavy tissue of high BMI patients with MFU-V, they may be better candidates for surgical intervention. Alternatively, they may achieve desired effects with multiple MFU-V treatments. Conversely, patients with a very low BMI may have skin laxity secondary to volume depletion. In these cases, volume restoration may be considered first and MFU-V as a secondary intervention.Other factors that contribute to poor outcomes include unrealistic expectations, as discussed above, and technical errors such as delivering MFU energy at incorrect tissue depths.
caused by smoking are associated with poor overall skin quality, which is less likely to achieve the same magnitude of response as healthy skin. To help counter this effect, some advisors provide oral nutritional supplements and vitamins, such as ascorbic acid (vitamin C) to counteract the damaging oxidative effects of smoking and maximize the beneficial effects of MFU-V.Another factor is a high body-mass index (BMI), especially for a single MFU-V treatment. As it is challenging to lift heavy tissue of high BMI patients with MFU-V, they may be better candidates for surgical intervention. Alternatively, they may achieve desired effects with multiple MFU-V treatments. Conversely, patients with a very low BMI may have skin laxity secondary to volume depletion. In these cases, volume restoration may be considered first and MFU-V as a secondary intervention.Other factors that contribute to poor outcomes include unrealistic expectations, as discussed above, and technical errors such as delivering MFU energy at incorrect tissue depths.Factors to Consider Prior to Treatment
Some individuals may not be ideal candidates for MFU-V due to underlying medical comorbidities. These include individualswith connective tissue disorders, immune deficiencies, or other disorders that may affect the normal healing and tissue remodeling processes. Similarly, chronic treatment with antiinflammatory or immunosuppressive medicines may affect how well patients heal from thermal injury.
Customized Treatment: Energy Levels and Line Counts
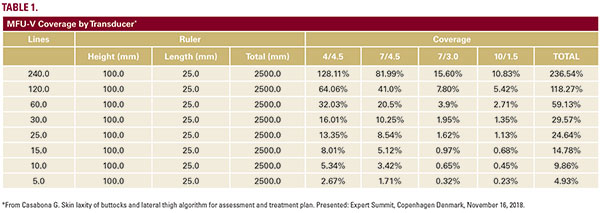
It was universally agreed the MFU-V energy setting should be set at the highest tolerable level, titrating down as needed for patient comfort. All participants were comfortable with providing treatment using multiple energy levels with no expectation of diminished results, provided proper treatment line density is maintained. Participants were not comfortable with proposing an upper or lower limit on number of lines for a full-face and neck treatment. It was agreed that a range of 800-1200 lines was reasonable, recognizing that the actual number and placement of lines is based on individualized needs, including the size of the patient’s face and the results of ultrasound visualization. Surface area covered by each transducer with the same number of lines are delivered in the same treatment area are provided in Table 1. Adjustments in number of lines can be made to provide the same amount of treatment coverage depending on transducer used.Visualization should always be performed to assess the depth of the SMAS relative to more superficial layers of the skin as these depths will influence transducer selection and planned number of lines at each depth.Treating at three depths is considered optimal, but it was acknowledged that many patients may not be good candidates for this approach because the measured depth of target tissues does not align with available transducers. To conserve the density thermal coagulation points, most experts suggested increasing the line count at two other treatment depths if one transducer is not used. Treating at a single depth is not recommended, as it is difficult to achieve the treatment density required for effectiveness without stacking too many thermal coagulation points at a single depth which may lead to adverse events.
Sequential Treatments to Optimize Outcomes
One of the meeting participants is currently performing an investigator-initiated study to assess the potential efficacy of sequential treatments performed 6 weeks apart to optimize the lifting results of MFU-V. The hypothesis behind this study is that the wound repair mechanism is still working within this time interval and performing additional treatments may capitalize on these ongoing processes. It was agreed that this was a safe approach, as prior evidence from studies that assessed the use of MFU-V for treating rosacea and acne scars used treatment in

