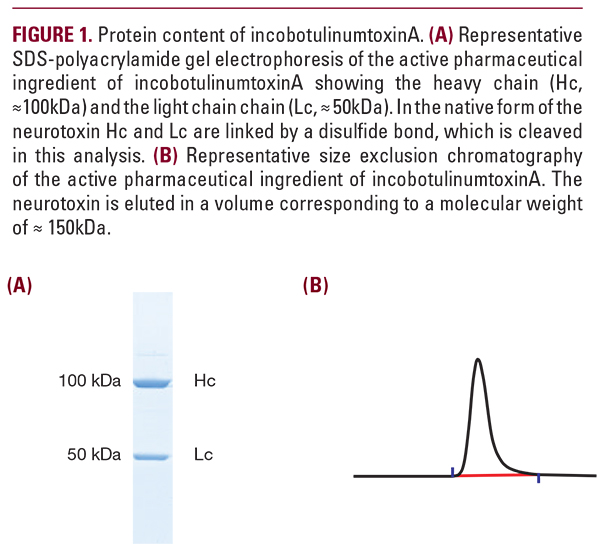
 (Figure 1), followed by the addition of excipients (sucrose and human serum albumin) and lyophilization.2 Stringent quality checks include visual inspection, vial weight checks, leak detection after 7-day hold, and ultraviolet light datametrics code application to confirm toxin identity. The unique and precise purification process of incobotulinumtoxinA ensures that only the active 150 kDa neurotoxin, needed to achieve the clinical effect, is included.18 IncobotulinumtoxinA contains no nucleic acid content, compared with onabotulinumtoxinA, which contains DNA fragments of the neurotoxin gene.40 OnabotulinumtoxinA has a molecular weight of 900 kDa including unnecessary clostridial proteins and BoNT-A.20 The exact molecular weight of the BoNT complex in abobotulinumtoxinA is unknown, but is accepted to be up to 900 kDa, with the 300 kDa protein complex as the most abundant.2 The specific activity of abobotulinumtoxinA, incobotulinumtoxinA, and onabotulinumtoxinA is reported as 154 U/ng, 227 U/ng, and 137 U/ng, respectively, based on the mean BoNT concentration in 100 U (0.65 ng, 0.44 ng, and 0.73 ng of the 150 kDa BoNT, respectively; Figure 2).41The high specific activity of incobotulinumtoxinA is consistent with no inactivation of the BoNT during purification.41 In comparison, as onabotulinumtoxinA is reported to contain 0.73 ng of neurotoxin protein, the low specific activity of onabotulinumtoxinA suggests that a proportion of BoNT protein is inactive.41 OnabotulinumtoxinA is manufactured by several precipitation and redissolution steps prior to the addition of excipients (sodium chloride [NaCl] and human serum albumin), and vacuum-dried,2 resulting in a thin film of the product. An early study demonstrates that NaCl concentration may affect BoNT stability during freeze-drying, resulting in BoNT denaturation.42 This may explain the lower specific activity of onabotulinumtoxinA compared with abobotulinumtoxinA and incobotulinumtoxinA.41 Denatured BoNT may increase the risk of an immune response, subsequent development of neutralizing antibodies, and potential secondary non-response to further treatment.2,43
(Figure 1), followed by the addition of excipients (sucrose and human serum albumin) and lyophilization.2 Stringent quality checks include visual inspection, vial weight checks, leak detection after 7-day hold, and ultraviolet light datametrics code application to confirm toxin identity. The unique and precise purification process of incobotulinumtoxinA ensures that only the active 150 kDa neurotoxin, needed to achieve the clinical effect, is included.18 IncobotulinumtoxinA contains no nucleic acid content, compared with onabotulinumtoxinA, which contains DNA fragments of the neurotoxin gene.40 OnabotulinumtoxinA has a molecular weight of 900 kDa including unnecessary clostridial proteins and BoNT-A.20 The exact molecular weight of the BoNT complex in abobotulinumtoxinA is unknown, but is accepted to be up to 900 kDa, with the 300 kDa protein complex as the most abundant.2 The specific activity of abobotulinumtoxinA, incobotulinumtoxinA, and onabotulinumtoxinA is reported as 154 U/ng, 227 U/ng, and 137 U/ng, respectively, based on the mean BoNT concentration in 100 U (0.65 ng, 0.44 ng, and 0.73 ng of the 150 kDa BoNT, respectively; Figure 2).41The high specific activity of incobotulinumtoxinA is consistent with no inactivation of the BoNT during purification.41 In comparison, as onabotulinumtoxinA is reported to contain 0.73 ng of neurotoxin protein, the low specific activity of onabotulinumtoxinA suggests that a proportion of BoNT protein is inactive.41 OnabotulinumtoxinA is manufactured by several precipitation and redissolution steps prior to the addition of excipients (sodium chloride [NaCl] and human serum albumin), and vacuum-dried,2 resulting in a thin film of the product. An early study demonstrates that NaCl concentration may affect BoNT stability during freeze-drying, resulting in BoNT denaturation.42 This may explain the lower specific activity of onabotulinumtoxinA compared with abobotulinumtoxinA and incobotulinumtoxinA.41 Denatured BoNT may increase the risk of an immune response, subsequent development of neutralizing antibodies, and potential secondary non-response to further treatment.2,43 Implications for Use in Aesthetic Medicine
The clinical and real-world efficacy of incobotulinumtoxinA is established in >200 peer-reviewed publications.44,45 IncobotulinumtoxinA is proven to effectively reduce upper facial lines for up to 4 months post-treatment,46-49 with a high level of subject satisfaction47,48 and no treatment-related serious AEs in a Phase III trial leading to upper facial lines approval in Europe.47 The safety profile of incobotulinumtoxinA was further confirmed in a pooled analysis of 13 prospective multicenter studies in aesthetic indications of crow’s feet, glabellar lines, and upper facial lines. Overall, the frequency of treatment-related AEs was low and analysis of repeat-dose studies suggested the incidence of AEs may decrease with repeated treatments over time.50 In incobotulinumtoxinA clinical studies, no previously BoNT-A naive subject developed neutralizing antibodies51-55 or demonstrated secondary lack of treatment response,50,52 even with doses up to 800 U in the treatment of upper-limb spasticity,52 consistent with the low immunogenicity of incobotulinumtoxinA. In the published literature, all subjects who developed neutralizing antibodies and secondary non-response after incobotulinumtoxinA treatment had received treatment with another BoNT formulation.51,56 IncobotulinumtoxinA may be the best choice for patients seeking long-term treatment with BoNT due to the lower risk of neutralizing antibodies, such as treatment-naive patients. Moreover, in some cases, the low immunogenicity of incobotulinumtoxinA may offer a renewed therapeutic effect in subjects with antibody-induced BoNT-A treatment non-response.57,58
New Entrants to the BoNT Commercial Market
The number of BoNT-A products available on the commercial markets worldwide continues to increase and two new entrants currently under review are planning to file FDA Biologics License Applications. PrabotulinumtoxinA is a similar version of onabotulinumtoxinA in terms of pharmacological development and manufacturing compared with currently approved formulations.19 The specific potency of prabotulinumtoxinA was recorded as 133 U/ng compared with 240 U/ng for incobotulinumtoxinA, with a high percentage of inactive neurotoxin,14 consistent with inactivation of the BoNT due to the presence of NaCl during drying,42 and the manufacturing process of onabotulinumtoxinA discussed above. DaxibotulinumtoxinA is a new BoNT-A formulation currently in clinical development for aesthetic (glabellar lines) and therapeutic (cervical dystonia and plantar fasciitis) indica-

