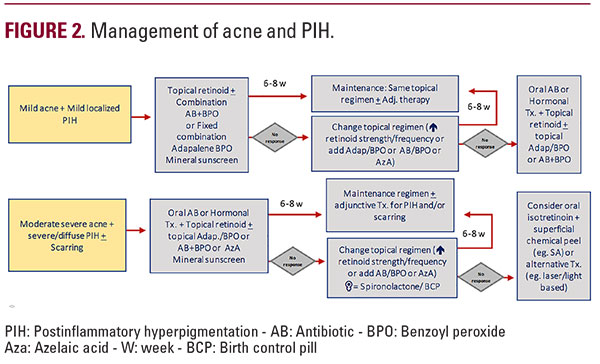
 Retinoids are considered the first line of topical treatment. In patients with a tendency to PIH, low concentration retinoids should be used, in cream, at bedtime, starting only 2 to 3 times a week until the skin tolerates them well. This also decreases the associated iatrogenic PIH.1,4-6 Fixed combinations like benzoyl peroxide with adapalene or benzoyl peroxide with clindamycin are used to treat mild to moderated papulopustular acne and help preventing PIH.1, 4-6 Azelaic acid 20% in cream is effective in the treatment of acne in Latin America and helps prevent PIH. In the United States, it is not indicated for the treatment of acne. It would be used off-label.1,4-6
Retinoids are considered the first line of topical treatment. In patients with a tendency to PIH, low concentration retinoids should be used, in cream, at bedtime, starting only 2 to 3 times a week until the skin tolerates them well. This also decreases the associated iatrogenic PIH.1,4-6 Fixed combinations like benzoyl peroxide with adapalene or benzoyl peroxide with clindamycin are used to treat mild to moderated papulopustular acne and help preventing PIH.1, 4-6 Azelaic acid 20% in cream is effective in the treatment of acne in Latin America and helps prevent PIH. In the United States, it is not indicated for the treatment of acne. It would be used off-label.1,4-6 Oral Treatment
Oral antibiotics (eg, doxycycline): First line of treatment for moderate to severe acne (papulopustular, nodulocystic); Should be used at the same time with benzoyl peroxide to prevent bacterial resistance.Oral Isotretinoin: For nodular-cystic or non-responsive to treatment acne. Should be started with low dose and increased progressively. Helps to prevent PIH.1,4-6 Hormonal therapy: For women; Oral contraceptives with antiandrogen properties (eg, Drospirenone or Norethindrone + ethinyl estradiol); Concomitant treatment for menstrual cycle-related inflammatory acne.Spironolactone: For women with menstrual cycle-related inflammatory acne.4-6
Adjuvant Therapy
Skin care: Mild cleanser with or without salicylic acid and with ceramides, cholesterol, and fatty acids to improve the damaged skin barrier; Non-comedogenic moisturizers and daily, fluid, UVA-UVB, non-comedogenic sunscreen; Avoid scrubs, alcohol-based toners, and exfoliating cleanser to prevent irritation.Chemical peels: Very superficial chemical peels with lactic acid, salicylic, or glycolic acid; Help to prevent and treat PIH; Preparation 2 to 3 weeks before the procedure with a combination of a bleaching agent like hydroquinone with retinoids and corticosteroids is mandatory.1,6  Rosacea: Clinical Considerations Rosacea is more frequent in patients with a background from the southern cone of South America (Argentina, Uruguay, Southern Brazil, Chile, and Paraguay) because their skin is lighter due to the presence of Italian and German immigrants after the first and second world wars. Although the disease is more common in phototype I and II (Fitzpatrick), it can also be suffered by people with darker skin color. It could be misdiagnosed with adult acne. To try to avoid this, we must consider rosacea in the differential diagnosis when we have a patient with darker skin, facial flushing, heat, eye symptoms, or papulopustular elements and absence of comedones.Four subtypes of rosacea can be diagnosed: Erythematotelangiectatic (ETR), papulopustular (PPR), glandular hyperplastic or phymatous rosacea (GH/FR), and ocular (OR). The granulomatous variant is more frequent in darker phototype skin.7,8 Unlike acne, postinflammatory hyperpigmentation is rare in patients with rosacea among patients with Latin American ancestry.8,9.
Rosacea: Clinical Considerations Rosacea is more frequent in patients with a background from the southern cone of South America (Argentina, Uruguay, Southern Brazil, Chile, and Paraguay) because their skin is lighter due to the presence of Italian and German immigrants after the first and second world wars. Although the disease is more common in phototype I and II (Fitzpatrick), it can also be suffered by people with darker skin color. It could be misdiagnosed with adult acne. To try to avoid this, we must consider rosacea in the differential diagnosis when we have a patient with darker skin, facial flushing, heat, eye symptoms, or papulopustular elements and absence of comedones.Four subtypes of rosacea can be diagnosed: Erythematotelangiectatic (ETR), papulopustular (PPR), glandular hyperplastic or phymatous rosacea (GH/FR), and ocular (OR). The granulomatous variant is more frequent in darker phototype skin.7,8 Unlike acne, postinflammatory hyperpigmentation is rare in patients with rosacea among patients with Latin American ancestry.8,9.
 Rosacea: Clinical Considerations Rosacea is more frequent in patients with a background from the southern cone of South America (Argentina, Uruguay, Southern Brazil, Chile, and Paraguay) because their skin is lighter due to the presence of Italian and German immigrants after the first and second world wars. Although the disease is more common in phototype I and II (Fitzpatrick), it can also be suffered by people with darker skin color. It could be misdiagnosed with adult acne. To try to avoid this, we must consider rosacea in the differential diagnosis when we have a patient with darker skin, facial flushing, heat, eye symptoms, or papulopustular elements and absence of comedones.Four subtypes of rosacea can be diagnosed: Erythematotelangiectatic (ETR), papulopustular (PPR), glandular hyperplastic or phymatous rosacea (GH/FR), and ocular (OR). The granulomatous variant is more frequent in darker phototype skin.7,8 Unlike acne, postinflammatory hyperpigmentation is rare in patients with rosacea among patients with Latin American ancestry.8,9.
Rosacea: Clinical Considerations Rosacea is more frequent in patients with a background from the southern cone of South America (Argentina, Uruguay, Southern Brazil, Chile, and Paraguay) because their skin is lighter due to the presence of Italian and German immigrants after the first and second world wars. Although the disease is more common in phototype I and II (Fitzpatrick), it can also be suffered by people with darker skin color. It could be misdiagnosed with adult acne. To try to avoid this, we must consider rosacea in the differential diagnosis when we have a patient with darker skin, facial flushing, heat, eye symptoms, or papulopustular elements and absence of comedones.Four subtypes of rosacea can be diagnosed: Erythematotelangiectatic (ETR), papulopustular (PPR), glandular hyperplastic or phymatous rosacea (GH/FR), and ocular (OR). The granulomatous variant is more frequent in darker phototype skin.7,8 Unlike acne, postinflammatory hyperpigmentation is rare in patients with rosacea among patients with Latin American ancestry.8,9. Treatment of Rosacea
General Care: Avoid trigger factors; Use daily, continuous sun-protection.


