


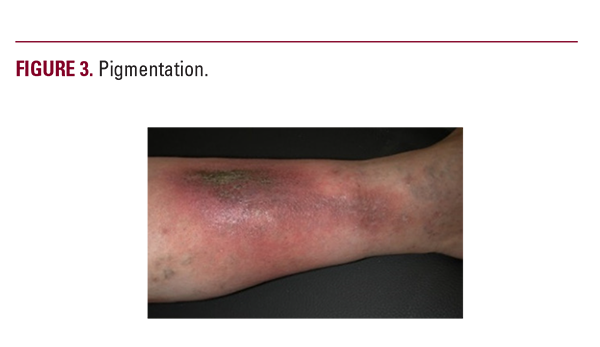
CVI may lead to spider veins, reticular varicose veins, and edema (Figure 1). CVI induces inflammation and skin changes such as xerosis (Figure 2), pigmentation (Figure 3), dermatitis (Figure 4), lipodermatosclerosis, atrophie blanche, and eventually, venous ulceration (Table 2).5,6,10,11 Venous ulcers can vary in size, can be difficult to manage and diminish quality of

life, particularly if they are painful, complicated with dermatitis and xerosis, or drain profusely.5,6,10-17 The management of leg ulcers is outside the scope of this review.
The prevalence of venous leg dermatitis (VLD) in patients >50 years in the US is estimated to be 6-7% (~15-20 million individuals), making this twice as prevalent as psoriasis.18,19 VLD presents initially as poorly demarcated erythematous plaques of the lower legs bilaterally, classically involving the medial malleolus.5-9 Duplex ultrasound is useful in demonstrating venous reflux to confirm the clinical diagnosis or when the clinical diagnosis of VLD is inadequate.5,7


