To the Editor,
Autoimmune blistering disorders (AIBD) are chronic, antibodymediated diseases of the skin and mucous membranes that carry substantial morbidity and mortality.1,2 Previous studies have suggested an association with malignancy, particularly squamous cell carcinoma and lymphoma, but have been limited by small sample sizes and subtype-specific cohorts.3 We conducted a population-based analysis using the TriNetX Research Network, a federated electronic health record database, to better define malignancy risk in this population.
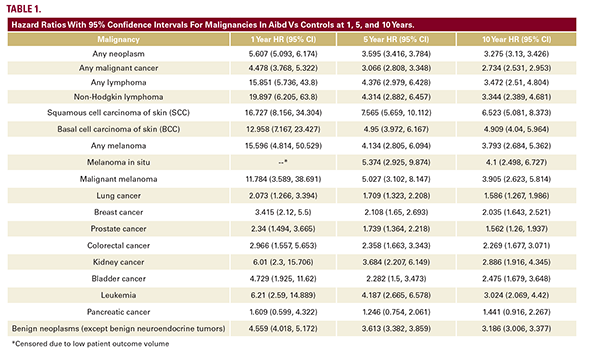
We conducted a retrospective cohort study using the TriNetX Research Network, a de-identified EHR database with longitudinal patient-level data from over 100 healthcare organizations. We identified adults with ICD-10 codes for pemphigus (L10), pemphigoid (L12), or other bullous disorders (L13) and excluded those with prior malignancy. The index date was the diagnosis of bullous disorder for our exposure cohort and a general exam encounter for controls; events >20 years prior were excluded. Patients were matched 1:1 to controls by demographics (age, sex, race), comorbidities (hypertension, diabetes, chronic respiratory disease, obesity, ischemic heart disease, chronic kidney disease, liver disease, heart failure, and nicotine dependence), family history of malignancy, and immunosuppression use, yielding 30,218 patients per group. Outcomes were assessed from one day post-index through 1, 5, and 10 years of follow up. Covariate balance was assessed via standardized mean differences, with all covariates achieving SMD <0.1. Absolute risks, risk differences (RD), Kaplan-Meier
Autoimmune blistering disorders (AIBD) are chronic, antibodymediated diseases of the skin and mucous membranes that carry substantial morbidity and mortality.1,2 Previous studies have suggested an association with malignancy, particularly squamous cell carcinoma and lymphoma, but have been limited by small sample sizes and subtype-specific cohorts.3 We conducted a population-based analysis using the TriNetX Research Network, a federated electronic health record database, to better define malignancy risk in this population.
We conducted a retrospective cohort study using the TriNetX Research Network, a de-identified EHR database with longitudinal patient-level data from over 100 healthcare organizations. We identified adults with ICD-10 codes for pemphigus (L10), pemphigoid (L12), or other bullous disorders (L13) and excluded those with prior malignancy. The index date was the diagnosis of bullous disorder for our exposure cohort and a general exam encounter for controls; events >20 years prior were excluded. Patients were matched 1:1 to controls by demographics (age, sex, race), comorbidities (hypertension, diabetes, chronic respiratory disease, obesity, ischemic heart disease, chronic kidney disease, liver disease, heart failure, and nicotine dependence), family history of malignancy, and immunosuppression use, yielding 30,218 patients per group. Outcomes were assessed from one day post-index through 1, 5, and 10 years of follow up. Covariate balance was assessed via standardized mean differences, with all covariates achieving SMD <0.1. Absolute risks, risk differences (RD), Kaplan-Meier