INTRODUCTION
Hand, foot, and mouth disease (HFMD) is a contagious viral infection most commonly caused by Coxsackievirus A16 (CVA16) and Enterovirus A71 (EVA71), members of the Enterovirus genus within the Picornaviridae family. Symptoms typically include fever, malaise, pharyngitis, and a papulovesicular rash, characteristically appearing on the hands, feet, groin/buttock, and mouth, which resolves in 7 to 10 days without intervention. Most cases are mild (86.2%) or asymptomatic (12.7%).1 A small percentage of cases develop neurological complications (eg, aseptic meningitis, encephalitis) and cardiopulmonary failure, with EVA71 and CVA6 more likely to cause severe disease in 1.1% and death in 0.03% of cases.1
Infection occurs primarily through fecal-oral transmission and direct contact with lesions. On average, symptoms begin 3 to 6 days post-exposure, and supportive care remains the standard of treatment. No antiviral therapy is standard. However, multiple case reports have indicated that early oral acyclovir can accelerate symptom resolution, particularly in prolonged or severe cases.2-6
We present the first published case of HFMD successfully treated with valacyclovir, a prodrug of acyclovir. Valacyclovir and acyclovir are antiviral drugs used to treat herpesvirus infections and are not recommended for HFMD due to the lack of viral thymidine kinase within the Enterovirus genus. Nonetheless, symptom overlap with herpesvirus infections has led to the empirical use of antivirals with unexpected clinical benefits.
CASE PRESENTATION
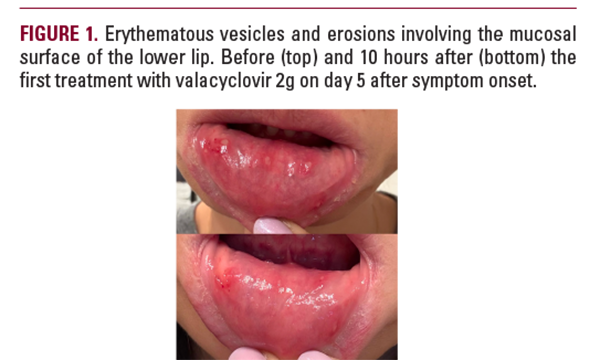
A 39-year-old healthy female developed tender vesicles and papules on her palms and soles. These symptoms began 7 days after her school-aged child developed similar symptoms, which were diagnosed as HFMD. On day 2, she developed herpangina and an increased number of acral blisters. The patient alternated over-the-counter oral acetaminophen and naproxen for analgesia. Symptoms progressed on day 4, with the emergence of a low-grade fever of 100.4°F, malaise, and worsening of oral and palmoplantar lesions. At 21:00 on day 4, she self-administered 2 g of valacyclovir. She awoke the next morning (day 5) with a significant reduction in pain and inflammation, then took 2 g of valacyclovir in the morning and 1 g at bedtime. Analgesia was no longer needed and was discontinued. There were no new lesions on day 6, and the patient was symptom-free. On day 7, she remained lesion-free, suggesting resolution ahead of the expected 7 to 10-day course.