INTRODUCTION
The appropriate size of surgical margins for stages after a positive Mohs micrographic surgery (MMS) stage has not been well studied. Proposed minimum peripheral margins (mPM) for excision can be determined using a mathematical model that describes the direct relationship between the extent of tissue block facing loss (FL) and the required mPM.
For Stage 1 MMS excisions, margins typically range from 2 to 3 mm, though they may vary from 1 mm to over 4 mm.1,2
Before the first tissue wafer is placed on a microscope slide during frozen section processing, tissue wafers are removed from the tissue block during the trimming or "facing" process. This FL discards a portion of the surgical margin. This may result in a deviation in position between the residual tumor's (RT's) actual location in the wound and the location where it is observed microscopically.
For Stage 1 MMS excisions, margins typically range from 2 to 3 mm, though they may vary from 1 mm to over 4 mm.1,2
Before the first tissue wafer is placed on a microscope slide during frozen section processing, tissue wafers are removed from the tissue block during the trimming or "facing" process. This FL discards a portion of the surgical margin. This may result in a deviation in position between the residual tumor's (RT's) actual location in the wound and the location where it is observed microscopically.
MATERIALS AND METHODS
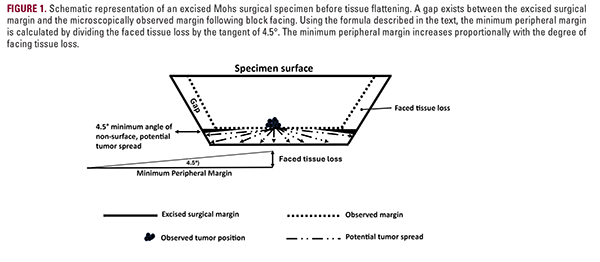
The mathematical approach used to determine mPM was developed by Dr Sharon Tiefenbrunn (now deceased). It is based on the trigonometric formula used to calculate the unknown side of a right triangle when the length of one side (the amount of FL) and the angle of the hypotenuse (the angle of tumor spread with respect to the surgical margin) are known. The unknown side length is the mPM. (Figure 1)
Formula
unknown side length (mPM) = (known side length (FL))
(tangent of hypotenuse angle)
Formula
unknown side length (mPM) = (known side length (FL))
(tangent of hypotenuse angle)
- A 180° arc encompasses all potential directions of RT extension. To ensure the subsequent stage excision encompasses RT, 95% of all potential angles and directions of RT extension should be included in the overlap of the RT focus. Including very shallow angles of tumor extension is not practical because angles less than 4.5 degrees result in an impractically larger calculation for mPM, and RT extension at extremely shallow angles to the surgical margin should be encompassed by the 95% calculated mPM.
- Assume 95% of RT extension is located within 95% of a 180° arc: 180° x 95% = 171°
- 180° - 171° = 9°
- 9° ÷ 2 = 4.5° is the 95% minimum angle of potential RT spread to each side of the tumor. This is the hypotenuse angle of the right triangle.
- The tangent of 4.5° = 0.079
- Therefore: mPM = FL/0.079
RESULTS
The authors calculated an FL of approximately 150 μm for their practices. In comparison, Taylor et al. reported FL values ranging from 187 μm to 338 μm.3
Using the formula above, the corresponding mPM values for FLs of 100 μm, 150 μm, 200 μm, 250 μm, 300 μm, and 350 μm are approximately 1.3 mm, 1.9 mm, 2.5 mm, 3.2 mm, 3.8 mm, and 4.4 mm, respectively. An mPM in the range of 1 to 4 mm would be appropriate, depending on the FL calculated by each MMS laboratory.
Using the formula above, the corresponding mPM values for FLs of 100 μm, 150 μm, 200 μm, 250 μm, 300 μm, and 350 μm are approximately 1.3 mm, 1.9 mm, 2.5 mm, 3.2 mm, 3.8 mm, and 4.4 mm, respectively. An mPM in the range of 1 to 4 mm would be appropriate, depending on the FL calculated by each MMS laboratory.
DISCUSSION
Before the first tissue wafer is placed on a microscope slide during MMS frozen section processing, multiple tissue wafers are removed from the tissue block during the trimming or "facing" process. This FL discards a portion of the true surgical margin. As a result, a deviation in position may exist between the RT's actual location in the wound and the location where it is observed microscopically (Figure 1).
Failing to consider this deviation between the observed and actual position of RT during the design of subsequent MMS stage excision margins may result in recurrences. A quantification of the relationship between FL and mPM would enhance both tumor control and normal tissue conservation during MMS.
The use of the mathematical formula for the tangent of a right triangle calculates an mPM that accounts for RT positional uncertainties created by FL.
Failing to consider this deviation between the observed and actual position of RT during the design of subsequent MMS stage excision margins may result in recurrences. A quantification of the relationship between FL and mPM would enhance both tumor control and normal tissue conservation during MMS.
The use of the mathematical formula for the tangent of a right triangle calculates an mPM that accounts for RT positional uncertainties created by FL.
Several studies have reported that mPM for first-stage MMS excisions ranges from 1 mm to >4 mm.1,2 However, there is a paucity of research addressing mPM in subsequent stages of MMS. Additionally, few studies have assessed the variability in FL among MMS laboratories.
Some MMS laboratories begin mounting tissue wafers on slides as soon as a minimal amount of tissue appears on the face of the tissue block, while others continue to trim the tissue block until a nearly complete tissue layer is exposed before placing the wafer on a microscope slide for examination by the Mohs surgeon. Based on FL considerations, the mathematical model presented suggests that the mPM for RT would typically range from 1 mm to 4 mm. Nonetheless, the use of margins under 2 mm for certain tumor types and anatomic sites may be oncologically inadvisable.
Jerrom and Varma4 surveyed 39 Mohs surgeons and found considerable variability in the FL required to achieve full-margin visualization. FL ranged from less than 100 μm to 800 μm, with 59% of respondents achieving complete margin representation within 200 μm. A FL of 200 μm corresponds to a calculated mPM of 2.5 mm.
Mohs surgeons may readily calculate the amount of FL in their laboratory by multiplying the thickness of each tissue wafer by the number of wafers discarded after tissue is first encountered during block facing until the first wafer is mounted on a microscope slide. This calculated FL can then be used to adjust the estimated mPM using the formula described above. Notably, Taylor et al.3 also demonstrated that the greater the FL, the more MMS stages were required to achieve clear margins. In practical terms, the formula calculations suggest that an mPM of 2 mm to 4 mm for RT excisions will ensure that 95% of all potential directions of tumor infiltration are included, thereby minimizing the risk of false-negative results. A larger mPM may be appropriate for aggressive tumor subtypes and tumors that have exhibited widespread infiltration in previous stages. These findings also suggest that using less than 2 mm mPM for tissue conservation may be oncologically inadvisable.
Some MMS laboratories begin mounting tissue wafers on slides as soon as a minimal amount of tissue appears on the face of the tissue block, while others continue to trim the tissue block until a nearly complete tissue layer is exposed before placing the wafer on a microscope slide for examination by the Mohs surgeon. Based on FL considerations, the mathematical model presented suggests that the mPM for RT would typically range from 1 mm to 4 mm. Nonetheless, the use of margins under 2 mm for certain tumor types and anatomic sites may be oncologically inadvisable.
Jerrom and Varma4 surveyed 39 Mohs surgeons and found considerable variability in the FL required to achieve full-margin visualization. FL ranged from less than 100 μm to 800 μm, with 59% of respondents achieving complete margin representation within 200 μm. A FL of 200 μm corresponds to a calculated mPM of 2.5 mm.
Mohs surgeons may readily calculate the amount of FL in their laboratory by multiplying the thickness of each tissue wafer by the number of wafers discarded after tissue is first encountered during block facing until the first wafer is mounted on a microscope slide. This calculated FL can then be used to adjust the estimated mPM using the formula described above. Notably, Taylor et al.3 also demonstrated that the greater the FL, the more MMS stages were required to achieve clear margins. In practical terms, the formula calculations suggest that an mPM of 2 mm to 4 mm for RT excisions will ensure that 95% of all potential directions of tumor infiltration are included, thereby minimizing the risk of false-negative results. A larger mPM may be appropriate for aggressive tumor subtypes and tumors that have exhibited widespread infiltration in previous stages. These findings also suggest that using less than 2 mm mPM for tissue conservation may be oncologically inadvisable.
DISCLOSURES
Drs Steinman, Schiro, and Portnoff have no potential or
perceived conflicts of interest or financial relationships relevant
to the content of this manuscript.
ACKNOWLEDGMENT
This article is dedicated to the memory of our late colleague and
teacher, Dr Sharon Tiefenbrunn, who developed the concept we
present and championed mathematical precision in the practice
of Mohs surgery.
REFERENCES
- Lane JE, Kent DE. Surgical margins in the treatment of nonmelanoma skin cancer and Mohs micrographic surgery. Curr Surg. 2005;62(5):518-526.
- Cerci FB, Kubo EM, Werner B, et al. Surgical margins required for basal cell carcinomas treated with Mohs micrographic surgery based on tumor features. J Am Acad Dermatol. 2020;83:493-500
- Taylor BR, Groover JA, Cook J. Facing the block and false positives in Mohs surgery: a retrospective study of 2,198 cases. Dermatol Surg. 2013;39:1662- 1670.
- Jerrom R, Varma S. Tissue processing in Mohs micrographic surgery: what is current UK practice? Br J Dermatol. 2021;185:104.
AUTHOR CORRESPONDENCE
Howard K. Steinman MD hksteinman@gmail.com

