INTRODUCTION
Practice Points
- Depigmented halos are not restricted to melanocytic lesions; SK can rarely display a halo and may clinically resemble melanoma.1,2
- Dermoscopy of seborrheic keratosis is characterized by features such as milia-like cysts, comedo-like openings, a cerebriform sulcus–gyrus pattern, moth-eaten borders with irregular peripheral indentations, and sharp demarcation.2 However, melanoma clues include blue-black/blue-white structures and an atypical network. Recognition of these patterns guides biopsy decisions.2,6
- In skin of color, overlapping dermoscopic findings (eg, clonal SK vs pigmented basal cell carcinoma) create diagnostic pitfalls, underscoring the need for biopsy when uncertain.3
- For vitiligo, phase 3 and randomized evidence support topical ruxolitinib cream and NB-UVB, with both modalities applicable to patients with richly pigmented skin.4,5
CASE PRESENTATION
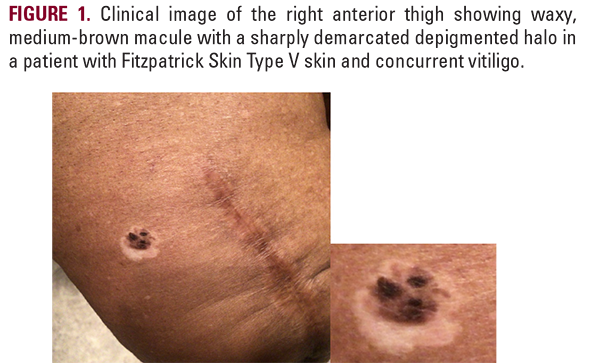
A 73-year-old woman with Fitzpatrick skin type V presented for progressive hypopigmentation. Depigmented patches began on the buttocks three years earlier, with later involvement of hands and feet. She also reported a stable, brownish-black, three-tone macule on the right anterior thigh present for nearly two decades, but within the past year, it developed an enlarging depigmented ring.
On examination, there was an 8-10 mm smooth, brownish-black, three-tone macule on the right anterior thigh that was encircled by a sharply bordered depigmented halo. Additional well-demarcated depigmented macules and patches were observed on the buttocks, hands, and feet.
A horizontal excision under local anesthesia was performed. Histopathology demonstrated classic SK morphology without atypia or malignancy, confirming a benign SK with a halo phenomenon.
The patient was reassured. Vitiligo management was discussed, including photoprotection, topical calcineurin inhibitors, NB-UVB phototherapy, and topical ruxolitinib 1.5% cream applied twice daily.4,5
On examination, there was an 8-10 mm smooth, brownish-black, three-tone macule on the right anterior thigh that was encircled by a sharply bordered depigmented halo. Additional well-demarcated depigmented macules and patches were observed on the buttocks, hands, and feet.
A horizontal excision under local anesthesia was performed. Histopathology demonstrated classic SK morphology without atypia or malignancy, confirming a benign SK with a halo phenomenon.
The patient was reassured. Vitiligo management was discussed, including photoprotection, topical calcineurin inhibitors, NB-UVB phototherapy, and topical ruxolitinib 1.5% cream applied twice daily.4,5