INTRODUCTION
Fixed drug eruption (FDE) is a common type of cutaneous adverse drug reaction that typically presents with the recurrence of single or multiple skin lesions at identical anatomical sites upon re-exposure to the offending agent. The most common triggers include antibiotics, non-steroidal anti-inflammatory drugs (NSAIDs), paracetamol, and anticonvulsants.1,2 Lesions most commonly appear within 48 hours of drug administration and are characterized by erythematous to violaceous, well-defined plaques featuring a distinctive dusky-grey center, often resulting in post-inflammatory hyperpigmentation.1,2 In some cases, patients can develop blisters, and, rarely, extensive skin detachment may occur, leading to a generalized bullous fixed drug eruption (GBFDE). GBFDE may be diagnosed when at least 10% of the body surface area is involved.1,3 GBFDE is classified as a severe cutaneous adverse reaction (SCAR), with a potential for fatal outcomes.4 Data and clinical experience regarding GBFDE are limited, particularly in the pediatric population.
CASE SUMMARY
A 14-year-old boy exhibited a 48-hour history of rapid-onset skin lesions. The patient presented with the medical history of Becker muscular dystrophy, diagnosed at the age of 5 years, then he developed focal epilepsy at the age of 9 years, and he had mild intellectual disability.
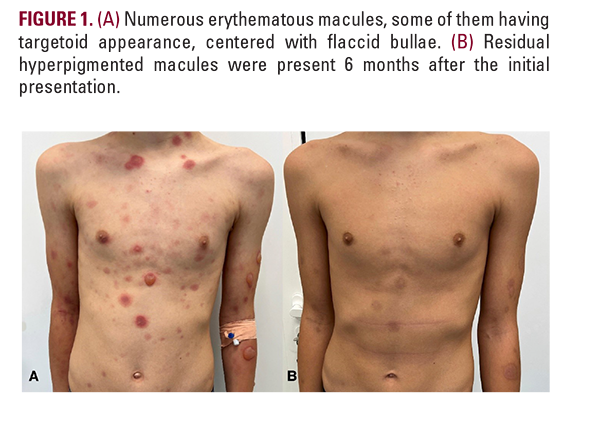
On admission, dusky-erythematous macules were present on his face, trunk, and extremities, centered by flaccid bullae, and some had targetoid features (Figure 1A). A larger lesion with an atrophic center was present in his mandibular region (Figure 2A). There was no mucosal involvement, and the patient was hemodynamically stable. Laboratory investigations revealed a mildly elevated erythrocyte sedimentation rate (32 mm/h).