INTRODUCTION
Minoxidil is a vasodilator used at higher doses as an anti-hypertensive, while low doses of oral minoxidil (LDOM) (between 0.25 and 5 mg) are effective in treating alopecia disorders. Rosacea is characterized by various subtypes, including erythematotelangiectatic, papulopustular, phymatous, and ocular.1
We have encountered patients with erythematotelangiectatic rosacea (ETR) who report flushing and worsening of their facial redness with use of LDOM (authors' unpublished data). To explore the association between ETR and use of LDOM, we analyzed real-world data, hypothesizing that use of vasodilatory medications like LDOM may disrupt cutaneous vascular homeostasis of ETR.
We have encountered patients with erythematotelangiectatic rosacea (ETR) who report flushing and worsening of their facial redness with use of LDOM (authors' unpublished data). To explore the association between ETR and use of LDOM, we analyzed real-world data, hypothesizing that use of vasodilatory medications like LDOM may disrupt cutaneous vascular homeostasis of ETR.
MATERIALS AND METHODS
Using TriNetX, we performed a retrospective study using anonymous electronic medical records. Patients diagnosed with "non scarring hair loss" (ICD-10 code L65) between 2005 and 2025 were 1:1 propensity score matched to patients with hair loss not treated with minoxidil (ICD-10 codes Z00.00 and Z00.129), based on age and race/ethnicity, using nearest-neighbor matching with a 0.1 caliper. Covariate balance post-matching was assessed via standardized mean differences (SMD), with SMD <0.1 indicating acceptable balance. This analysis compared the outcomes of two cohorts: Cohort A (58,099 patients, hair loss plus minoxidil) and Cohort B (892,040 patients, hair loss minus minoxidil).
Logistic regression framework calculated odds ratios (OR), risk ratios (RR), and risk differences (RD) to assess the association between minoxidil use and rosacea, a disease of capillaries, rhinophyma, other rosacea, rosacea conjunctivitis, and flushing. Wald 95% confidence intervals were computed, and statistical significance was defined as P<0.05 using two-sided z-tests.
Logistic regression framework calculated odds ratios (OR), risk ratios (RR), and risk differences (RD) to assess the association between minoxidil use and rosacea, a disease of capillaries, rhinophyma, other rosacea, rosacea conjunctivitis, and flushing. Wald 95% confidence intervals were computed, and statistical significance was defined as P<0.05 using two-sided z-tests.
RESULTS
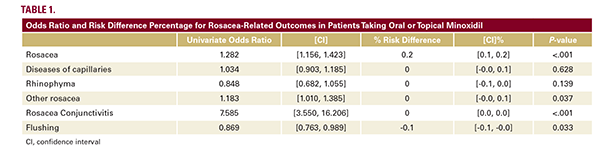
Compared with matched controls, individuals using minoxidil (topical and oral) for ‘other non-scarring hair loss’ had significantly higher odds of rosacea (OR 1.282; 95% CI, 1.156–1.423), other rosacea (OR 1.183; 95% CI, 1.010–1.385), and rosacea conjunctivitis (OR 7.585; 95% CI, 3.550–6.206) (Table 1). After adjusting for covariates, diseases of capillaries (P=0.628), perioral dermatitis (P=0.232), and rhinophyma (P=0.139) were not statistically significant (Table 1). All other comorbidities were statistically significant in univariate and multivariate analysis (P<0.05; Table 1).
DISCUSSION
Physiologically, minoxidil causes arteriolar vasodilation2; though the exact mechanism of hair regrowth is unknown, it is speculated that the vasodilatory properties contribute to increased oxygen, blood, and nutrient delivery to the hair follicle.3 Rosacea is a condition primarily affecting the face, causing flushing and redness. Dysregulation of cutaneous blood flow and upregulation of vasodilatory molecules may contribute to the disease.1 Minoxidil use and rosacea exacerbation may be