INTRODUCTION
Patients with inflammatory alopecias face a potentially greater risk of cutaneous neoplasms in affected areas, likely due to chronic inflammation and reduced hair coverage.1 While there have been isolated reports of scalp non-melanoma skin cancers (NMSC), particularly among women with lichen planopilaris (LPP), comprehensive evidence from large-scale studies is lacking.2 To assess the risk for subsequent scalp NMSCs in LPP patients, we conducted a retrospective cohort study using data extracted from a global anonymized healthcare network (TriNetX Network, 2005-2025).
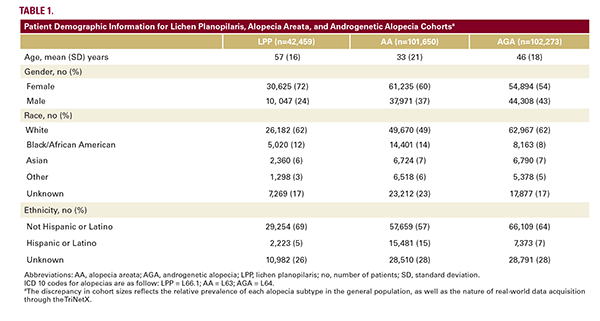
Three distinct alopecia cohorts were created, based on the specificity of ICD codes: LPP, androgenetic alopecia (AGA), and alopecia areata (AA), for comparative analysis.3 Each alopecia cohort was matched with a healthy control for age, sex, race, and ethnicity. Odds ratios (OR) were calculated to evaluate risk for subsequent skin cancers, including basal cell carcinoma (BCC), squamous cell carcinoma (SCC), malignant melanoma (MM), and melanoma in situ (MIS) (Tables 1 and 2).
Across all cohorts, women (LPP 72%, AA 60%, AGA 54%) and white patients were predominant (LPP 62%, AA 49%, AGA 62%; Table 1). Patients with LPP exhibited a significantly heightened likelihood of developing subsequent scalp and neck NMSCs (BCC: OR 2.03, CI 1.67-2.48; SCC: OR 2.03, CI 1.53-2.71) compared to controls (Table 2). LPP patients also had an increased risk of NMSC on all body sites, but no significant associations with MM or MIS. In comparison, patients with AA demonstrated modestly increased risks for SCC, while those with AGA showed a lower risk specifically for scalp and neck BCC. Interestingly, both the AA and AGA cohorts demonstrated protective effects against MM/MIS overall, not mirrored in the LPP cohort.
These findings suggest an association between LPP and increased risk of subsequent NMSCs, which was not observed in the AA and AGA cohorts. We could not verify the clinical observation that NMSCs predominantly manifest in affected scalp areas, primarily due to constraints imposed by the ICD code merging "neck and scalp" into a singular anatomical
Three distinct alopecia cohorts were created, based on the specificity of ICD codes: LPP, androgenetic alopecia (AGA), and alopecia areata (AA), for comparative analysis.3 Each alopecia cohort was matched with a healthy control for age, sex, race, and ethnicity. Odds ratios (OR) were calculated to evaluate risk for subsequent skin cancers, including basal cell carcinoma (BCC), squamous cell carcinoma (SCC), malignant melanoma (MM), and melanoma in situ (MIS) (Tables 1 and 2).
Across all cohorts, women (LPP 72%, AA 60%, AGA 54%) and white patients were predominant (LPP 62%, AA 49%, AGA 62%; Table 1). Patients with LPP exhibited a significantly heightened likelihood of developing subsequent scalp and neck NMSCs (BCC: OR 2.03, CI 1.67-2.48; SCC: OR 2.03, CI 1.53-2.71) compared to controls (Table 2). LPP patients also had an increased risk of NMSC on all body sites, but no significant associations with MM or MIS. In comparison, patients with AA demonstrated modestly increased risks for SCC, while those with AGA showed a lower risk specifically for scalp and neck BCC. Interestingly, both the AA and AGA cohorts demonstrated protective effects against MM/MIS overall, not mirrored in the LPP cohort.
These findings suggest an association between LPP and increased risk of subsequent NMSCs, which was not observed in the AA and AGA cohorts. We could not verify the clinical observation that NMSCs predominantly manifest in affected scalp areas, primarily due to constraints imposed by the ICD code merging "neck and scalp" into a singular anatomical