In skin of color, halo phenomena can mask benign lesions; biopsy and dermoscopic‑pathologic correlation remain essential
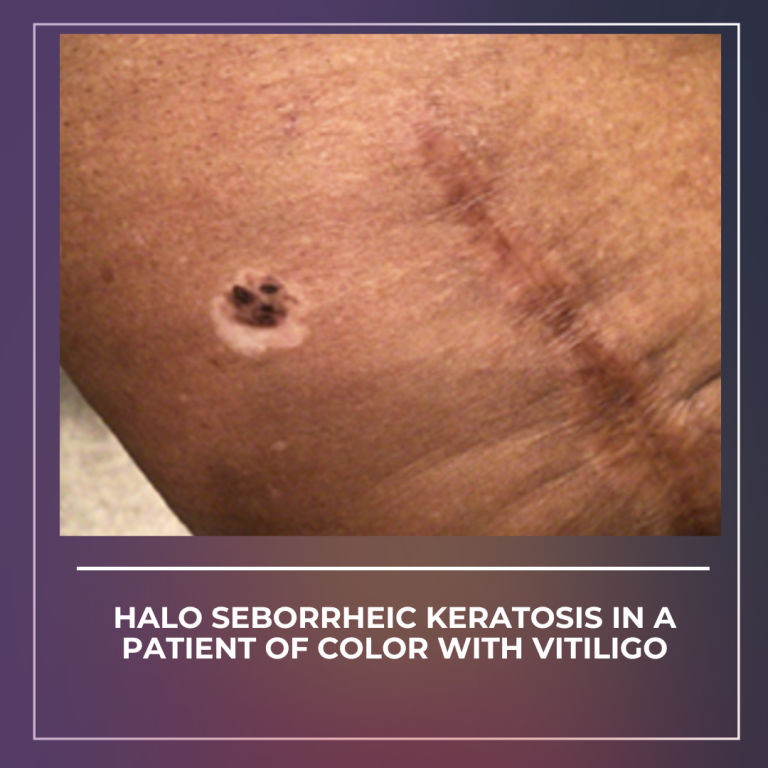
It’s time to dive into one of our January JDD case reports ! A 73‑year‑old woman with Fitzpatrick V, presented with a long‑standing, three‑tone brown‑black macule on the anterior thigh that developed a sharply demarcated depigmented halo, alongside depigmented patches consistent with vitiligo. Surgical excision and histology confirmed seborrheic keratosis without atypia, illustrating that the halo sign can occur around non‑melanocytic lesions and may mimic melanoma in richly pigmented skin. The case underscores the need to integrate dermoscopic clues with clinical history and to maintain a low threshold for histopathologic confirmation when the halo appearance is new, evolving, or atypical. It also reviews how dermoscopic and pathologic features help distinguish halo SK from melanoma and adult‑onset halo nevus, and summarizes practical options for coexisting vitiligo management (topical ruxolitinib 1.5% cream, narrowband UVB among them).
Call to action: When you encounter a new halo lesion, confirm with dermoscopy and consider biopsy or excision rather than assuming benignity.
Read the full case for the dermoscopic‑pathologic red flags and treatment pearls for concurrent vitiligo.
J Drugs Dermatol. 2026;25(1). doi:10.36849/JDD.9523
Blog write-up assisted by AI

