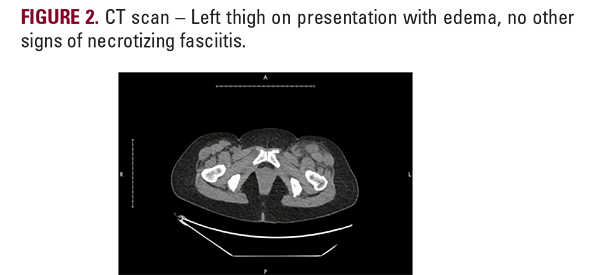
INTRODUCTION
Necrotizing fasciitis is an uncommon but potentially rapidly fatal infection. The mortality rate is estimated to be 23-29%1 and when it affects the limbs, the amputation rate is 11-14%.1 There are 4 types of necrotizing fasciitis: Type 1 (polymicrobial in immunocompromised patients), type 2 (group A streptococcus [GAS] in healthy people), type 3 (gas gangrene due to clostridium), and type 4 (marine organisms and fungal infections). Notably, necrotizing fasciitis type 2 (NF2) associated with GAS is associated with septic shock and multiorgan failure, and therefore, early recognition and treatment are critical to a good prognosis.2 Delays in diagnosis are unfortunately common due to the nonspecific nature of cutaneous signs and symptoms, radiological findings that lag behind the progressive and extensive soft tissue destruction, and the low frequency with which first responders and primary care and emergency medicine physicians encounter this entity.3,4
We report a case of NF2 that firstly benefited from early diagnosis and treatment, which resulted in a favorable outcome, and secondly demonstrated unexpected oral antibiotic failure due to a GAS M-protein variant.
Case Report
A previously healthy 50-year-old woman presented to the emergency room with severe pain in her left thigh for 4 days, limited weight-bearing capacity, and associated fever, fatigue, general body aches, and diarrhea. The patient did not report a history of injury to the affected area, nor any observed visible changes prior to presentation. Recent past medical history was pertinent for tonsillitis approximately 10 days preceding the leg pain, empirically treated with a 7-day course of amoxicillin/clavulanate potassium. There was no microbiological confirmation of GAS with a throat swab. The patient did not report any other new medications nor any history of illicit drug use. The patient did not report any other new medications nor any history of illicit drug use.
We report a case of NF2 that firstly benefited from early diagnosis and treatment, which resulted in a favorable outcome, and secondly demonstrated unexpected oral antibiotic failure due to a GAS M-protein variant.
Case Report
A previously healthy 50-year-old woman presented to the emergency room with severe pain in her left thigh for 4 days, limited weight-bearing capacity, and associated fever, fatigue, general body aches, and diarrhea. The patient did not report a history of injury to the affected area, nor any observed visible changes prior to presentation. Recent past medical history was pertinent for tonsillitis approximately 10 days preceding the leg pain, empirically treated with a 7-day course of amoxicillin/clavulanate potassium. There was no microbiological confirmation of GAS with a throat swab. The patient did not report any other new medications nor any history of illicit drug use. The patient did not report any other new medications nor any history of illicit drug use.

On examination, the left leg revealed minimal erythema (Figure 1) and was exquisitely tender to palpation on the medial aspectof the left thigh. The patient was initially normotensive on arrival, but suddenly developed tachycardia (120 bpm) and hypotension (79/50 mmHg). Initial labs revealed white cell count to be 17.1K/UL and serum creatinine to be 4.6 mg/dL, though the bloodcultures were negative. The presumed diagnosis was acuterenal failure associated with sepsis of unknown origin, though the disproportionate soft tissue pain raised the possibility of necrotizing fasciitis. Broad-spectrum antibiotics, including vancomycin, piperacillin-tazobactam, and clindamycin wereinitiated. Ultrasound of the left thigh was within normal limits,and a CT scan demonstrated soft tissue edema in the anterioraspect of her left thigh (Figure 2). Surgical exploration of her thigh revealed edema localized to the sartorius muscle with no