To the Editor,
Pseudofolliculitis barbae (PFB) is a chronic inflammatory disease caused by penetration of a shaved, curved hair shaft into the skin via extrafollicular or transfollicular mechanisms, most often affecting the neckline, cheeks, and chin in men and hair-bearing areas in women.1 The chronic inflammation associated with PFB often results in papules and pustules, secondary infection, post-inflammatory hyperpigmentation (PIH), and hypertrophic scarring.2,3 PFB can have a negative impact on quality of life, which can be exacerbated in individuals who are required to shave frequently due to occupational policies.4,5 While the dermatologic sequelae of PFB have been well documented, there are limited large-scale retrospective cohort studies that quantify the burden of secondary skin complications such as PIH and hypertrophic scarring, and investigate racial differences in time-to-treatment initiation for topical therapies.
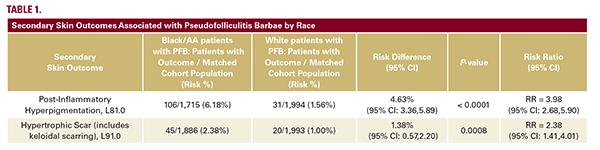
The TriNetX Research Network (>131 million patients) was queried on November 10th, 2025. Adults aged ≥ 18 years with ≥ 2 ICD-10 codes for PFB documented at least 1 month apart were included. 6,988 patients met diagnostic criteria, of which 2,113 identified as White and 4,031 as Black/African American (Black/ AA). After propensity score matching for age, sex, and gender, 2,045 patients were included within each cohort. All reported risk differences (RD) and relative risks (RR) are statistically significant (P<0.05). Black/AA patients had a significantly higher risk of secondary skin complications compared with White patients (Table 1), consistent with existing literature.1-3 PIH occurred in 6.18% of Black/AA patients vs.1.56% of White patients (RD=4.63%; RR=3.98). Hypertrophic scarring was observed in 2.38% of Black/ AA patients vs. 1.00% of White patients, (RD=1.38%; RR=2.38).
Time-to-treatment using topical medications for PFB varied by race (Table 2). Black/AA patients received topical corticosteroids sooner (281 ± 512 days) compared to White patients (352 ± 550 days), however White patients were more likely to receive them as initial therapy (36.5% vs. 28.4%). With regards to topical clindamycin, White patients had a shorter time to initiation (111 ± 272 days) compared to Black/AA (139 ± 340 days), and more frequently received it as initial treatment (26.7% vs. 18.6%). Black/AA patients received topical retinoids sooner (106 ± 294 days vs. 207 ± 439 days for White patients) and were prescribed them more frequently (13.1% vs. 9.98%). Time to benzoyl peroxide use was similar between groups, with similar frequency of use. Topical erythromycin was rarely used as it was not observed among White patients and was rarely used among Black/AA patients.
Pseudofolliculitis barbae (PFB) is a chronic inflammatory disease caused by penetration of a shaved, curved hair shaft into the skin via extrafollicular or transfollicular mechanisms, most often affecting the neckline, cheeks, and chin in men and hair-bearing areas in women.1 The chronic inflammation associated with PFB often results in papules and pustules, secondary infection, post-inflammatory hyperpigmentation (PIH), and hypertrophic scarring.2,3 PFB can have a negative impact on quality of life, which can be exacerbated in individuals who are required to shave frequently due to occupational policies.4,5 While the dermatologic sequelae of PFB have been well documented, there are limited large-scale retrospective cohort studies that quantify the burden of secondary skin complications such as PIH and hypertrophic scarring, and investigate racial differences in time-to-treatment initiation for topical therapies.
The TriNetX Research Network (>131 million patients) was queried on November 10th, 2025. Adults aged ≥ 18 years with ≥ 2 ICD-10 codes for PFB documented at least 1 month apart were included. 6,988 patients met diagnostic criteria, of which 2,113 identified as White and 4,031 as Black/African American (Black/ AA). After propensity score matching for age, sex, and gender, 2,045 patients were included within each cohort. All reported risk differences (RD) and relative risks (RR) are statistically significant (P<0.05). Black/AA patients had a significantly higher risk of secondary skin complications compared with White patients (Table 1), consistent with existing literature.1-3 PIH occurred in 6.18% of Black/AA patients vs.1.56% of White patients (RD=4.63%; RR=3.98). Hypertrophic scarring was observed in 2.38% of Black/ AA patients vs. 1.00% of White patients, (RD=1.38%; RR=2.38).
Time-to-treatment using topical medications for PFB varied by race (Table 2). Black/AA patients received topical corticosteroids sooner (281 ± 512 days) compared to White patients (352 ± 550 days), however White patients were more likely to receive them as initial therapy (36.5% vs. 28.4%). With regards to topical clindamycin, White patients had a shorter time to initiation (111 ± 272 days) compared to Black/AA (139 ± 340 days), and more frequently received it as initial treatment (26.7% vs. 18.6%). Black/AA patients received topical retinoids sooner (106 ± 294 days vs. 207 ± 439 days for White patients) and were prescribed them more frequently (13.1% vs. 9.98%). Time to benzoyl peroxide use was similar between groups, with similar frequency of use. Topical erythromycin was rarely used as it was not observed among White patients and was rarely used among Black/AA patients.