INTRODUCTION
Angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) are among the most commonly prescribed antihypertensives worldwide.1 While these agents are effective in managing hypertension, recent studies suggest that modulation of the renin-angiotensin-aldosterone system (RAAS) may influence cutaneous wound healing, angiogenesis, and fibrosis.1-3 Nearly half of adults have a diagnosis of hypertension, and approximately 35% of all prescriptions written for antihypertensive medications in the United States are for ACEi.4,5 With the prevalence of hypertension as a worldwide medical comorbidity and the rising incidence of cutaneous neoplasms in an aging population, understanding the perioperative effects of commonly used medications such as ACEis and ARBs, which inhibit the RAAS system, is increasingly important. This study aims to evaluate the association between ACEi/ARB use and perioperative complications in patients undergoing Mohs micrographic surgery (MMS).
MATERIALS AND METHODS
A global retrospective cohort study was conducted utilizing TriNetX, a database containing records from over 120 million patients across 80 health care organizations worldwide. Adults (greater than or equal to 18 years) who underwent MMS were identified using ICD-10 codes and stratified by the presence of an active prescription for an ACEi or ARB at the time of surgery. Propensity score matching (PSM) was performed to control for potential confounders, including age, sex, comorbidities (eg, diabetes, CKD, cardiovascular disease), and concurrent medication use. Analysis of risk and overall survival (OS) between cohorts was undertaken, examining the likelihood of developing intraoperative or postprocedural complications within 30 days after MMS. A 5-year OS analysis was conducted using the Kaplan-Meier method. Statistical significance was defined at two-tailed P-values < 0.05.
RESULTS
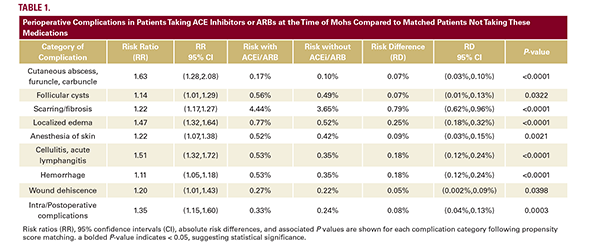
After PSM, we identified 102,242 patients taking ACEis/ARBs and a matched cohort not on these medications at the time of MMS.