INTRODUCTION
Photodermatoses are disorders characterized by abnormal cutaneous reactions to ultraviolet radiation (UVR) or visible light.1 They are categorized as idiopathic, endogenous, or due to exogenous agents.1 Idiopathic photodermatoses include polymorphic light eruption, juvenile spring eruption, hydroa vacciniforme-like lymphoproliferative disorder, actinic prurigo, chronic actinic dermatitis, and solar urticaria.1,2 Among the idiopathic photodermatoses, polymorphic light eruption is the most common, with an estimated prevalence of 10% among the general population.3 The pathophysiology is thought to result from UVR triggering immune dysregulation, resulting in autoimmunity and development of erythematous papules, vesicles, or plaques within hours of sun exposure with associated itch and/or burning.2,4 Endogenous photodermatoses are inherently phototoxic disorders. They primarily comprise the porphyrias, which are genetic disorders in heme metabolism that lead to porphyrin accumulation. Upon UVR exposure, affected individuals may develop photosensitivity, crusted lesions, bullae, and scarring.1,5
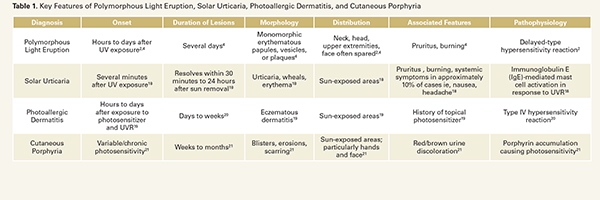
Exogenous photodermatoses are classified as phototoxic or photoallergic reactions.1 Phototoxic reactions occur when a drug or chemical absorbs UVR and directly damages skin cells, leading to exaggerated sunburn-like erythema, edema, or blistering.1,6 Common causative agents include sparfloxacin, doxycycline, ciprofloxacin, voriconazole, hydrochlorothiazide, naproxen, and other non-steroidal anti-inflammatory drugs.6 In contrast, photoallergic reactions are immune-mediated, delayed hypersensitivity responses that develop only in previously sensitized individuals.1 A recent analysis of photopatch testing in 363 patients with suspected photoallergic contact dermatitis (PACD) identified a 20% PACD prevalence, with sunscreens containing benzophenones, antimicrobials, and fragrances as the most common allergens.1 Key features of photodermatoses are summarized in Table 1.
Photodermatoses have substantial impacts on quality of life and daily practices such as clothing choices, employment, and social life, underscoring the need for adequate treatment.7
In the absence of standardized management guidelines, this review summarizes current photodermatoses therapies and highlights emerging preventive and treatment strategies.
Photodermatoses Management
Prevention
While sunscreens primarily protect against UVR by absorbing or reflecting radiation, formulations that combine physical filters, such as titanium dioxide and iron oxide, with DNA repair enzymes, including photolyase and endonuclease, enhance photoprotection in patients with photodermatoses.1,8 Physical filters provide broadspectrum UVR and visible light protection, while DNA repair enzymes help reverse UV-induced DNA damage.1,8
Oral and topical photoprotective adjuvants have gained attention for their ability to prevent UV damage and may benefit patients with photodermatoses. Polypodium leucotomos extract (PLE) is derived from the Polypodium leucotomos fern and has an extensive
Exogenous photodermatoses are classified as phototoxic or photoallergic reactions.1 Phototoxic reactions occur when a drug or chemical absorbs UVR and directly damages skin cells, leading to exaggerated sunburn-like erythema, edema, or blistering.1,6 Common causative agents include sparfloxacin, doxycycline, ciprofloxacin, voriconazole, hydrochlorothiazide, naproxen, and other non-steroidal anti-inflammatory drugs.6 In contrast, photoallergic reactions are immune-mediated, delayed hypersensitivity responses that develop only in previously sensitized individuals.1 A recent analysis of photopatch testing in 363 patients with suspected photoallergic contact dermatitis (PACD) identified a 20% PACD prevalence, with sunscreens containing benzophenones, antimicrobials, and fragrances as the most common allergens.1 Key features of photodermatoses are summarized in Table 1.
Photodermatoses have substantial impacts on quality of life and daily practices such as clothing choices, employment, and social life, underscoring the need for adequate treatment.7
In the absence of standardized management guidelines, this review summarizes current photodermatoses therapies and highlights emerging preventive and treatment strategies.
Photodermatoses Management
Prevention
While sunscreens primarily protect against UVR by absorbing or reflecting radiation, formulations that combine physical filters, such as titanium dioxide and iron oxide, with DNA repair enzymes, including photolyase and endonuclease, enhance photoprotection in patients with photodermatoses.1,8 Physical filters provide broadspectrum UVR and visible light protection, while DNA repair enzymes help reverse UV-induced DNA damage.1,8
Oral and topical photoprotective adjuvants have gained attention for their ability to prevent UV damage and may benefit patients with photodermatoses. Polypodium leucotomos extract (PLE) is derived from the Polypodium leucotomos fern and has an extensive