INTRODUCTION
Endocrine therapy, including aromatase inhibitors (AIs) and tamoxifen, and human epidermal growth factor receptor 2 (HER2)-targeted therapy, have significantly improved breast cancer outcomes, reducing mortality and prolonging disease-free survival.1-3
AIs block aromatase-mediated conversion of androgens to estrogens in peripheral tissues, making them particularly effective in postmenopausal women.4 Commonly used third-generation agents include anastrozole and letrozole (nonsteroidal) and exemestane (steroidal).³
Anti-HER2 monoclonal antibodies trastuzumab and pertuzumab downregulate HER2 signaling and induce immune-mediated tumor cell death, and are standard therapy for HER2-overexpressing tumors.5
While generally well tolerated, AIs may cause hot flashes, arthralgias, alopecia, pruritus, xerosis, hypersensitivity, vasculitis, and lichenoid eruptions.6-11 Trastuzumab’s common toxicities include diarrhea and dermatitis;¹² but rarer dermatologic adverse events (dAEs) like psoriasis, dermatomyositis, acneiform eruptions, and pigmentary changes are described.13-19 Despite their implications for treatment adherence and quality of life, dAEs remain poorly characterized.
Case 1: A 57-year-old woman with stage IIb ER+/HER2+ breast cancer developed painful papules and pustules on her face days after starting adjuvant letrozole. Topical metronidazole and ketoconazole were ineffective; doxycycline provided little benefit until letrozole was discontinued, after which lesions resolved rapidly.
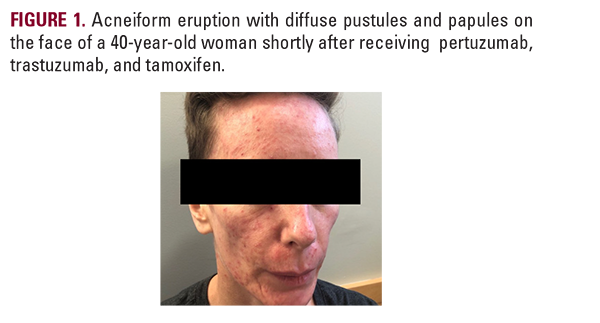
Case 2: A 40-year-old woman receiving pertuzumab, trastuzumab, and tamoxifen developed inflammatory papules and pustules on the face and neck within 2 weeks (Figure 1). Multiple topical and oral agents failed; isotretinoin achieved near clearance in 5 months without interrupting anti-HER2 therapy.
AIs block aromatase-mediated conversion of androgens to estrogens in peripheral tissues, making them particularly effective in postmenopausal women.4 Commonly used third-generation agents include anastrozole and letrozole (nonsteroidal) and exemestane (steroidal).³
Anti-HER2 monoclonal antibodies trastuzumab and pertuzumab downregulate HER2 signaling and induce immune-mediated tumor cell death, and are standard therapy for HER2-overexpressing tumors.5
While generally well tolerated, AIs may cause hot flashes, arthralgias, alopecia, pruritus, xerosis, hypersensitivity, vasculitis, and lichenoid eruptions.6-11 Trastuzumab’s common toxicities include diarrhea and dermatitis;¹² but rarer dermatologic adverse events (dAEs) like psoriasis, dermatomyositis, acneiform eruptions, and pigmentary changes are described.13-19 Despite their implications for treatment adherence and quality of life, dAEs remain poorly characterized.
Case 1: A 57-year-old woman with stage IIb ER+/HER2+ breast cancer developed painful papules and pustules on her face days after starting adjuvant letrozole. Topical metronidazole and ketoconazole were ineffective; doxycycline provided little benefit until letrozole was discontinued, after which lesions resolved rapidly.
Case 2: A 40-year-old woman receiving pertuzumab, trastuzumab, and tamoxifen developed inflammatory papules and pustules on the face and neck within 2 weeks (Figure 1). Multiple topical and oral agents failed; isotretinoin achieved near clearance in 5 months without interrupting anti-HER2 therapy.