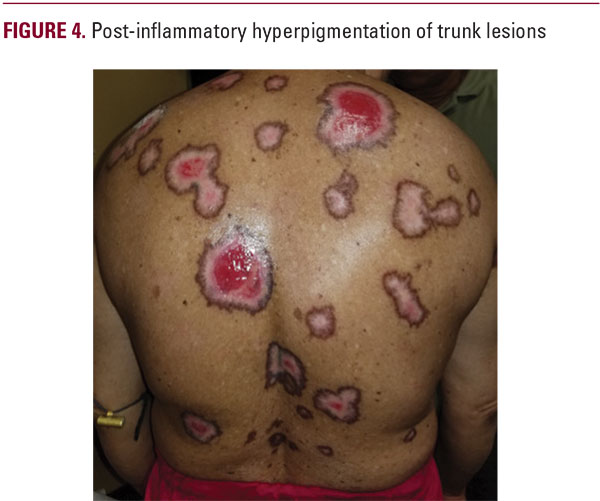
 history of radiation or tobacco exposure and no unintentional weight loss. Her past medical history includes hypertension, liver disease, hyperlipidemia, and diabetes mellitus. She has no known allergies. The patient takes metformin/sitagliptin, glimepiride, vitamin D3, hydrochlorothiazide, metoprolol, and pravastatin as scheduled. She has no family history of skin cancer and no other prior personal history of skin cancer.The decision was rendered to begin 5-fluouracil cream 5% applied to the affected areas twice a day, three times a week, as well as nicotinamide 500 mg po tid. Persistence of consummate wound care (ie, Vaseline to wounds, non-stick Xeroform gauze) was emphasized to the patient’s husband, who would be administering her medications. Given the large body surface area involved, we elected to monitor CBC and CMP.At future follow up visits, the patient’s skin lesions began to resolve. Her chemistry panels remained stable and were unremarkable. Her husband reported that she never missed a dose of 5-fluorouracil. A yellow, loosely adherent crust formed over her lesions that was removed, causing discomfort during the procedure but allowed for subsequent re-epithelialization of the 5-FU-induced erosions. Two months after her first encounter, the patient’s lesions had all completely resolved with post-inflammatory pigment alteration (Figure 4), except for those on her palms, soles, and scalp, where 5-FU was not applied. We will consider oral acitretin for her acral lesions and a trial of 5-FU cream 5% for her scalp lesion at a future date.
history of radiation or tobacco exposure and no unintentional weight loss. Her past medical history includes hypertension, liver disease, hyperlipidemia, and diabetes mellitus. She has no known allergies. The patient takes metformin/sitagliptin, glimepiride, vitamin D3, hydrochlorothiazide, metoprolol, and pravastatin as scheduled. She has no family history of skin cancer and no other prior personal history of skin cancer.The decision was rendered to begin 5-fluouracil cream 5% applied to the affected areas twice a day, three times a week, as well as nicotinamide 500 mg po tid. Persistence of consummate wound care (ie, Vaseline to wounds, non-stick Xeroform gauze) was emphasized to the patient’s husband, who would be administering her medications. Given the large body surface area involved, we elected to monitor CBC and CMP.At future follow up visits, the patient’s skin lesions began to resolve. Her chemistry panels remained stable and were unremarkable. Her husband reported that she never missed a dose of 5-fluorouracil. A yellow, loosely adherent crust formed over her lesions that was removed, causing discomfort during the procedure but allowed for subsequent re-epithelialization of the 5-FU-induced erosions. Two months after her first encounter, the patient’s lesions had all completely resolved with post-inflammatory pigment alteration (Figure 4), except for those on her palms, soles, and scalp, where 5-FU was not applied. We will consider oral acitretin for her acral lesions and a trial of 5-FU cream 5% for her scalp lesion at a future date.DISCUSSION
The above case illustrates the treatment of squamous cell carcinoma in situ induced by excessive exposure to arsenic using a regimen consisting of topical 5-FU and oral nicotinamide. The response to treatment was excellent, with complete resolution of lesions to which the cream was applied. We speculate that the nicotinamide did not contribute a large role in cure, but it was prescribed on the basis of its reported beneficial effects in preventing actinic keratosis.10 We attribute success of this therapy in large part to the diligent and consistent application of medication and wound care by the patient’s husband.Many topical and oral treatment modalities exist for treating arsenical keratosis, including 5-fluorouracil (5-FU), which acts by decreasing DNA synthesis in rapidly dividing cells, imiquimod, which induces an inflammatory surge, and acitretin, which decreases abnormal cellular proliferation.3 As displayed by Sharma et al, a similar response rate to ours was achieved in a patient with arsenic-induced SCC in situ; however, these authors used a combination therapy consisting of topical 5-FU and acitretin.5 Basaran et al demonstrated the potential benefits of a monotherapy, but their agent of choice was solely topical acitretin.6 A separate study mirrored the results of Basaran; however, they chose to use oral acitretin instead of a topical preparation.8 Finally, a paper by Youn et al demonstrated the elimination of SCC in situ using topical 5-FU while adding a surgical element and etretinate to their protocol.7 One of the most important lessons gleaned from this case is the value that proper care outside of the clinical setting has on patient outcomes. The patient’s spouse was not only very attentive to his wife’s needs, but knowledgeable as to how to properly administer her care. This implies that it is crucial for physicians to take extensive measures to ensure that patients and their caregivers understand how to handle their conditions at home. This is especially true for dermatology, as a large amount of our treatment actively takes place outside of the office and our specialty has historically reported low compliance rates to topical medication application.9
CONCLUSION
In conclusion, this case highlights the importance of patient compliance when treating multiple arsenical keratoses and the utility of topical 5-FU 5% in the eradication of extensive disease.

