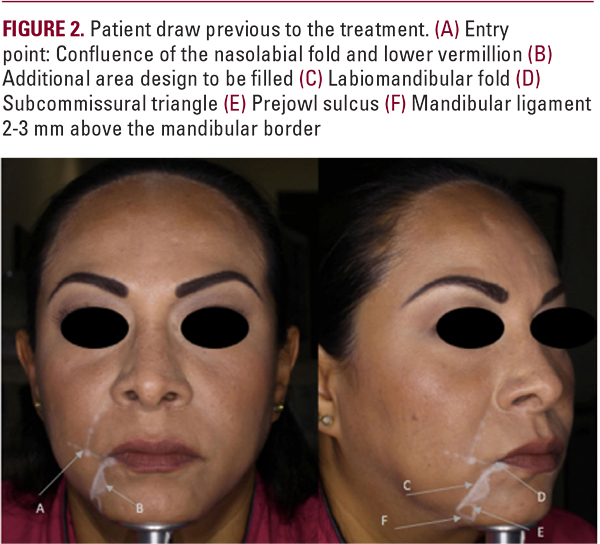
The DAO and the depressor labii inferioris (DLI) have been demonstrated to have strong miodermal attachments for mimicry and facial expression. The continuous movement is the cause of many of the lines, creases, and irregularities found in the inferior perioral skin.Taking these points into consideration, we propose a subcision technique using a cannula that separates the skin from the labiomandibular ligament and part of the DAO and DLI muscles. The subcised area smooths out the skin, while simultaneously allows one to design a subdermal space that can be safety filled to achieve evenness and regularity in the perioral area. Another benefit is that the subcision and separation of the labiomandibular fold from the oral commissure allows the oral commissure from being pulled downward and to achieve a more upward position. Finally, if needed, the prejowl sulcus can also be directly treated at the end of the procedure.Happy Face Technique If the lower third of the face is recognized as an area requiring treatment for beautification purposes after a personalized facial assessment, a Happy Face treatment is suggested. The main conceptual basis of the Happy Face procedure is the separation of the skin from the depressor muscles to also create a plane to be filled with hyaluronic acid (HA) of medium to high G’ with good product tissue integration7 using the cannula as a subcision tool. The authors used Restylene Volyme or Restylene Define as these hyaluronic acids fulfilled the preceding desired qualities.The initial step in the Happy Face procedure is marking the patient. For this purpose, the jowl is pushed forward and the marionette line is marked. A subcommissural triangle is also drawn and further labiomental areas that have irregularities that need to be subcised are also marked (Figure 2). Inferiorly the mandibular ligament is drawn 2 mm above the mandibular border and the area of the prejowl sulcus is outlined. The entry point for the cannula is marked by the crossing of a line extending laterally from the lower vermillion and the nasolabial fold on each side. This location is very useful because there are no important underlying vascular structures rendering this entry point relatively safe. There is a good superficial fat compartment facilitating sliding the cannula subdermally. In addition, one can direct the cannula superiorly and treat the nasolabial fold if desired from the same insertion point.The authors prefer a 25 G cannula (Softfill precision cannula), introduced and slid subdermally towards the oral commissure until touching the labiomandibular ligament. Taking the tissue between two fingers, the cannula is softly pushed through the ligament back and forth until a subcision of the labiomandibular ligament starting from the oral commissure for a length of 5-10mm inferiorly is completed. Subcision of the pre-marked areas medial to the labiomandibular fold are then done. The pre-jowl sulcus is not subsized. Once the area is fully liberated and the cannula can be easily displaced side to side, the HA is injected until complete smoothing of the area is attained. Soft massage can be done as well.