Treatment was initiated with imiquimod 5% cream five times weekly and mupirocin 2% ointment two times weekly. At theeight-week follow up for possible surgical resection, the lesion was completely resolved with no adverse events (Figure 1b).
DISCUSSION
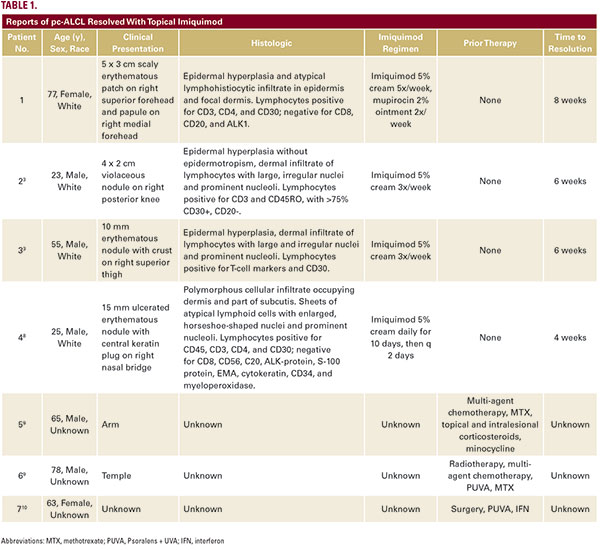
Pc-ALCL is a CD30+ T-cell subtype of CTCL. Clinically, it presents with primary or multiple erythematous papules or nodules, mostcommonly on the leg.2 Pc-ALCL affects males more frequently than females (3:1), with a median age of diagnosis of 55 years. It has an indolent clinical course and five-year survival rate of 85- 100%. Diffuse skin involvement, initial presentation on the head and neck, and extensive disease on a single limb are associated with a worse prognosis.2Histologically, pc-ALCL is characterized by a dense dermal infiltrate comprised of >75% CD30+ lymphocytes with paleeosinophilic cytoplasm.3 Most are positive for CD4 and demonstrate loss of CD2, CD3, and CD5. T-cell receptor gene translocations are observed in most cases.The differential diagnosis for pc-ALCL includes systemic ALCL with cutaneous involvement, lymphomatoid papulosis (LyP), and CD30+ mycosis fungoides (MF). Compared to systemic